Michael Siev, Audrey Renson, Hung-Jui Tan, Tracy L Rose, Stella K Kang, William C Huang, Marc A Bjurlin
{"title":"Prognostic Value of Histologic Subtype and Treatment Modality for T1a Kidney Cancers.","authors":"Michael Siev, Audrey Renson, Hung-Jui Tan, Tracy L Rose, Stella K Kang, William C Huang, Marc A Bjurlin","doi":"10.3233/kca-190072","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>To evaluate overall survival (OS) of T1a kidney cancers stratified by histologic subtype and curative treatment including partial nephrectomy (PN), percutaneous ablation (PA), and radical nephrectomy (RN).</p><p><strong>Materials and methods: </strong>We queried the National Cancer Data Base (2004-2015) for patients with T1a kidney cancers who were treated surgically. OS was estimated by Kaplan-Meier curves based on histologic subtype and management. Cox proportional regression models were used to determine whether histologic subtypes and management procedure predicted OS.</p><p><strong>Results: </strong>46,014 T1a kidney cancers met inclusion criteria. Kaplan Meier curves demonstrated differences in OS by treatment for clear cell, papillary, chromophobe, and cystic histologic subtypes (all <i>p</i> < 0.001), but no differences for sarcomatoid (<i>p</i> = 0.110) or collecting duct (<i>p</i> = 0.392) were observed. Adjusted Cox regression showed worse OS for PA than PN among patients with clear cell (HR 1.58, 95%CI [1.44-1.73], papillary RCC (1.53 [1.34-1.75]), and chromophobe RCC (2.19 [1.64-2.91]). OS was worse for RN than PN for clear cell (HR 1.38 [1.28-1.50]) papillary (1.34 [1.16-1.56]) and chromophobe RCC (1.92 [1.43-2.58]). Predictive models using Cox proportional hazards incorporating histology and surgical procedure alone were limited (c-index 0.63) while adding demographics demonstrated fair predictive power for OS (c-index 0.73).</p><p><strong>Conclusions: </strong>In patients with pathologic T1a RCC, patterns of OS differed by surgery and histologic subtype. Patients receiving PN appears to have better prognosis than both PA and RN. However, the incorporation of histologic subtype and treatment modality into a risk stratification model to predict OS had limited utility compared with variables representing competing risks.</p>","PeriodicalId":74039,"journal":{"name":"Kidney cancer (Clifton, Va.)","volume":"4 1","pages":"49-58"},"PeriodicalIF":1.1000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8171275/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney cancer (Clifton, Va.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3233/kca-190072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/3/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: To evaluate overall survival (OS) of T1a kidney cancers stratified by histologic subtype and curative treatment including partial nephrectomy (PN), percutaneous ablation (PA), and radical nephrectomy (RN).
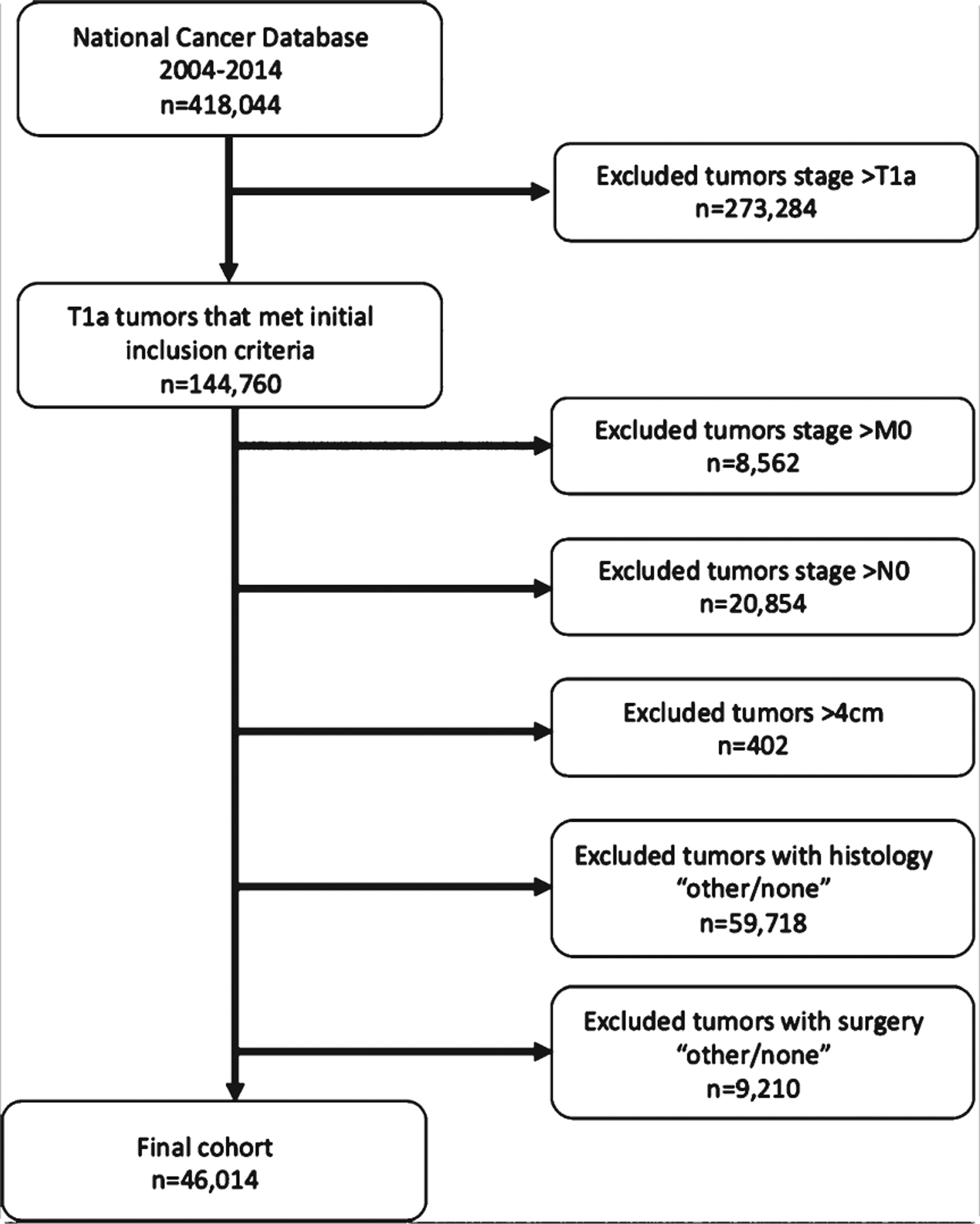
Materials and methods: We queried the National Cancer Data Base (2004-2015) for patients with T1a kidney cancers who were treated surgically. OS was estimated by Kaplan-Meier curves based on histologic subtype and management. Cox proportional regression models were used to determine whether histologic subtypes and management procedure predicted OS.
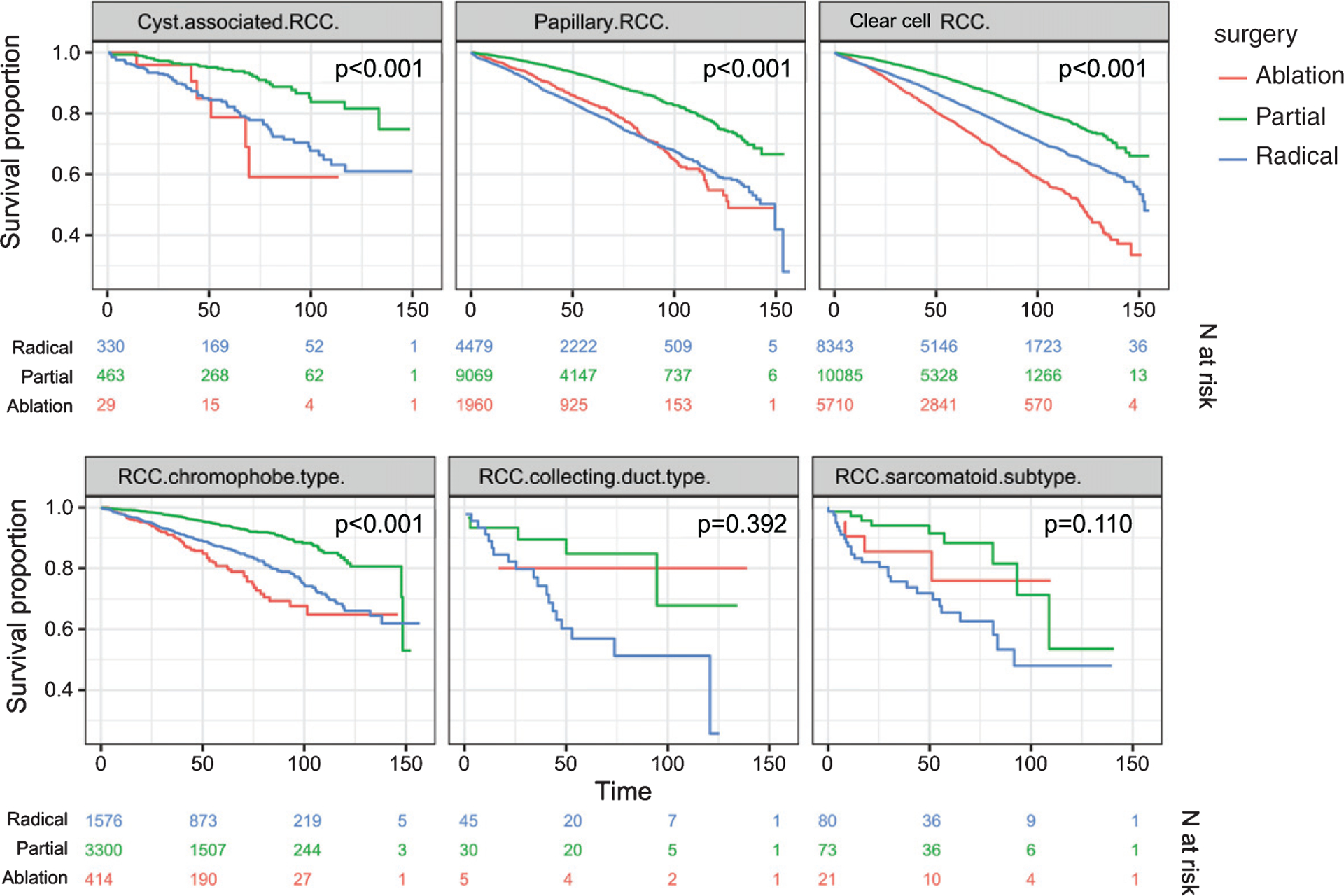
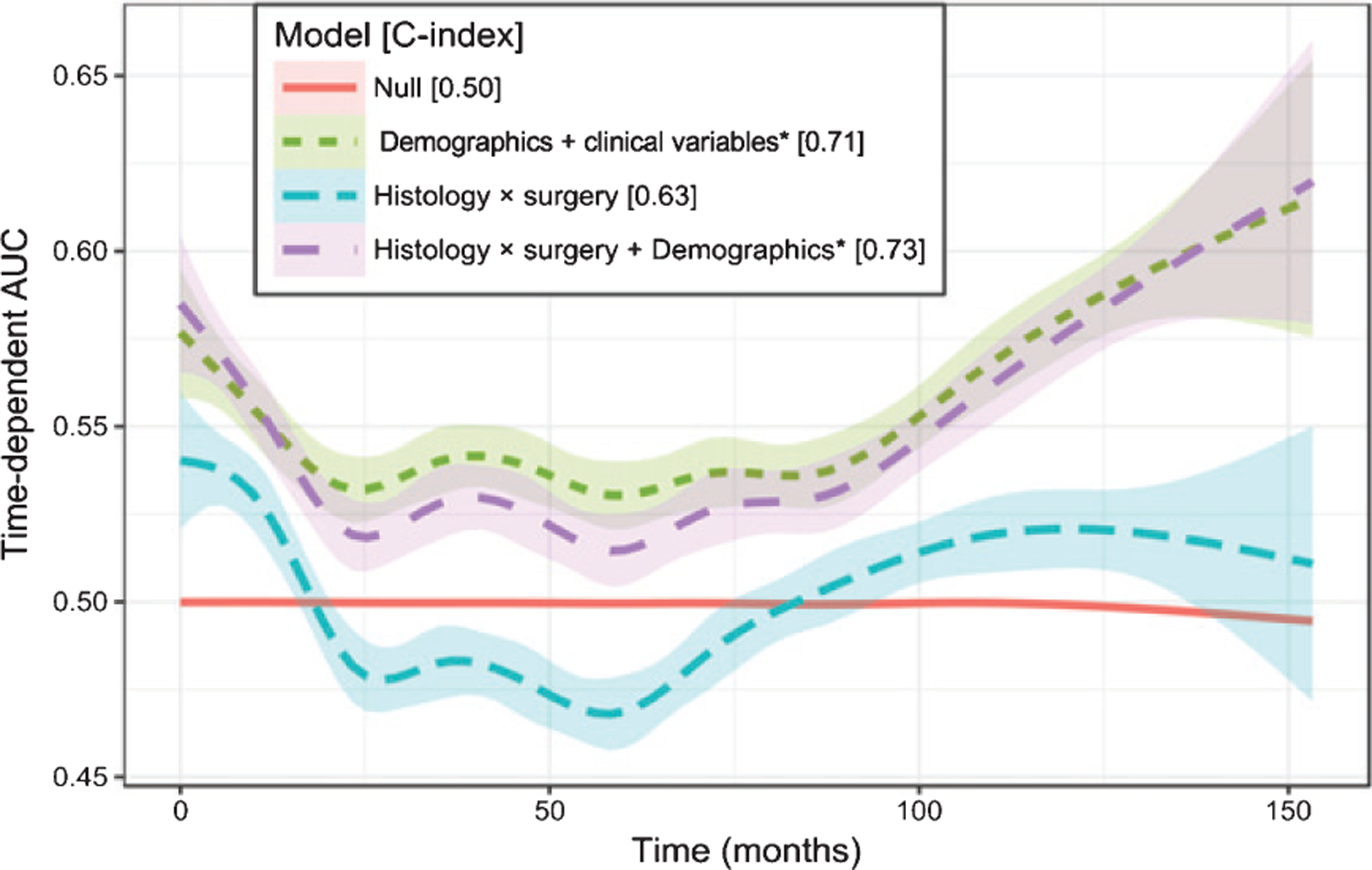
Results: 46,014 T1a kidney cancers met inclusion criteria. Kaplan Meier curves demonstrated differences in OS by treatment for clear cell, papillary, chromophobe, and cystic histologic subtypes (all p < 0.001), but no differences for sarcomatoid (p = 0.110) or collecting duct (p = 0.392) were observed. Adjusted Cox regression showed worse OS for PA than PN among patients with clear cell (HR 1.58, 95%CI [1.44-1.73], papillary RCC (1.53 [1.34-1.75]), and chromophobe RCC (2.19 [1.64-2.91]). OS was worse for RN than PN for clear cell (HR 1.38 [1.28-1.50]) papillary (1.34 [1.16-1.56]) and chromophobe RCC (1.92 [1.43-2.58]). Predictive models using Cox proportional hazards incorporating histology and surgical procedure alone were limited (c-index 0.63) while adding demographics demonstrated fair predictive power for OS (c-index 0.73).
Conclusions: In patients with pathologic T1a RCC, patterns of OS differed by surgery and histologic subtype. Patients receiving PN appears to have better prognosis than both PA and RN. However, the incorporation of histologic subtype and treatment modality into a risk stratification model to predict OS had limited utility compared with variables representing competing risks.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
