Bioactive glass S53P4 vs. autologous bone graft for filling defects in patients with chronic osteomyelitis and infected non-unions - a single center experience.
Eva Steinhausen, Rolf Lefering, Martin Glombitza, Nikolaus Brinkmann, Carsten Vogel, Bastian Mester, Marcel Dudda
{"title":"Bioactive glass S53P4 vs. autologous bone graft for filling defects in patients with chronic osteomyelitis and infected non-unions - a single center experience.","authors":"Eva Steinhausen, Rolf Lefering, Martin Glombitza, Nikolaus Brinkmann, Carsten Vogel, Bastian Mester, Marcel Dudda","doi":"10.5194/jbji-6-73-2021","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b>: The goals of osteomyelitis therapy are successful control of infection and reconstruction of the bone. The gold standard for filling defects is the autologous bone graft. Bioactive glass S53P4 is an inorganic bone substitute. We compared the outcome of using bioactive glass (BAG) versus autologous bone graft (AB) in patients with infected non-union. <b>Methods</b>: Patients with chronic osteomyelitis and infected non-union who received either bioactive glass or autologous bone grafts between 2013 and 2017 were analyzed retrospectively. The primary endpoint was successful control of infection during follow-up. Secondary endpoints were bone healing, functional outcome, and occurrence of complications. <b>Results</b>: Eighty-three patients were analyzed (BAG <math><mrow><mi>n</mi> <mo>=</mo> <mn>51</mn></mrow> </math> , AB <math><mrow><mi>n</mi> <mo>=</mo> <mn>32</mn></mrow> </math> ). Twenty-one patients experienced reinfection (BAG <math><mrow><mi>n</mi> <mo>=</mo> <mn>15</mn></mrow> </math> , 29 %; AB <math><mrow><mi>n</mi> <mo>=</mo> <mn>6</mn></mrow> </math> , 19 %). Seventy-eight patients achieved full weight bearing (BAG <math><mrow><mi>n</mi> <mo>=</mo> <mn>47</mn></mrow> </math> , 92 %; AB <math><mrow><mi>n</mi> <mo>=</mo> <mn>31</mn></mrow> </math> , 97 %). Sixty-four patients had complete bone healing at the end of the follow-up period (BAG <math><mrow><mi>n</mi> <mo>=</mo> <mn>39</mn></mrow> </math> , 77 %; AB <math><mrow><mi>n</mi> <mo>=</mo> <mn>25</mn></mrow> </math> , 78 %). There were no significant differences between the groups with respect to the primary or secondary endpoints. Patients with multidrug-resistant pathogens had a significantly higher rate of incomplete bone healing ( <math><mrow><mi>p</mi> <mo>=</mo> <mn>0</mn></mrow> </math> .033) and a 3-fold higher risk of complications in both groups. <b>Conclusions</b>: Bioactive glass appears to be a suitable bone substitute not only for successful control of infection and defect filling but also for bone healing in cases of infected non-union. In our study, bioactive glass was neither superior nor inferior to autologous bone graft with regard to the primary and secondary endpoints. Further studies with larger numbers of patients are required.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"6 4","pages":"73-83"},"PeriodicalIF":2.8000,"publicationDate":"2021-01-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8132459/pdf/","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-6-73-2021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 8
Abstract
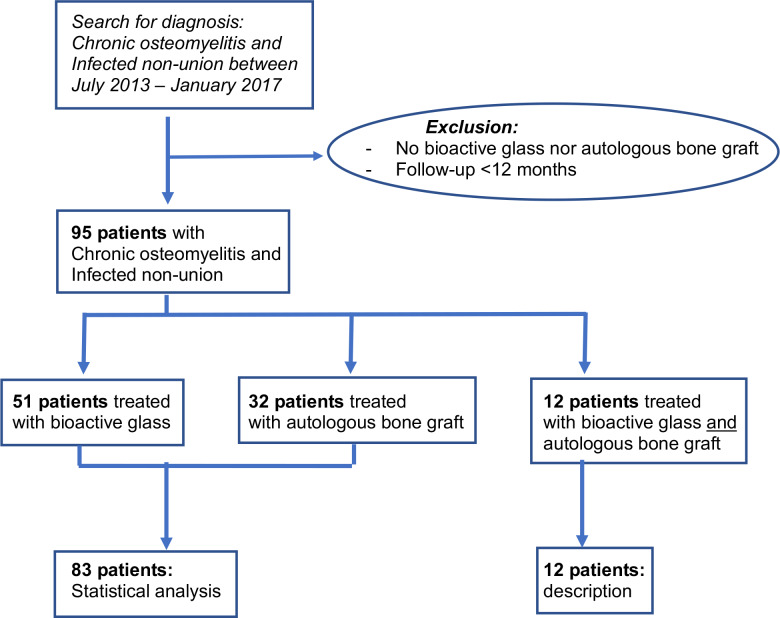
Introduction: The goals of osteomyelitis therapy are successful control of infection and reconstruction of the bone. The gold standard for filling defects is the autologous bone graft. Bioactive glass S53P4 is an inorganic bone substitute. We compared the outcome of using bioactive glass (BAG) versus autologous bone graft (AB) in patients with infected non-union. Methods: Patients with chronic osteomyelitis and infected non-union who received either bioactive glass or autologous bone grafts between 2013 and 2017 were analyzed retrospectively. The primary endpoint was successful control of infection during follow-up. Secondary endpoints were bone healing, functional outcome, and occurrence of complications. Results: Eighty-three patients were analyzed (BAG , AB ). Twenty-one patients experienced reinfection (BAG , 29 %; AB , 19 %). Seventy-eight patients achieved full weight bearing (BAG , 92 %; AB , 97 %). Sixty-four patients had complete bone healing at the end of the follow-up period (BAG , 77 %; AB , 78 %). There were no significant differences between the groups with respect to the primary or secondary endpoints. Patients with multidrug-resistant pathogens had a significantly higher rate of incomplete bone healing ( .033) and a 3-fold higher risk of complications in both groups. Conclusions: Bioactive glass appears to be a suitable bone substitute not only for successful control of infection and defect filling but also for bone healing in cases of infected non-union. In our study, bioactive glass was neither superior nor inferior to autologous bone graft with regard to the primary and secondary endpoints. Further studies with larger numbers of patients are required.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
