Characteristics and Surgical Results of Patients with Hypertrophic Obstructive Cardiomyopathy without Intrinsic Mitral Valve Diseases Undergoing Mitral Subvalvular Procedures during Myectomy.
Qiang Ji, YuLin Wang, Ye Yang, LiMin Xia, WenJun Ding, Kai Song, ChunSheng Wang
{"title":"Characteristics and Surgical Results of Patients with Hypertrophic Obstructive Cardiomyopathy without Intrinsic Mitral Valve Diseases Undergoing Mitral Subvalvular Procedures during Myectomy.","authors":"Qiang Ji, YuLin Wang, Ye Yang, LiMin Xia, WenJun Ding, Kai Song, ChunSheng Wang","doi":"10.1155/2020/8875405","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mitral subvalvular procedures have acquired a major role during hypertrophic obstructive cardiomyopathy (HOCM) surgery. However, few studies have focused on characterizing the clinical feature of HOCM patients without intrinsic mitral valve (MV) diseases undergoing mitral subvalvular procedures in addition to myectomy. Additionally, scant data about the results of mitral subvalvular procedures during HOCM surgery are available. This single-center study aims to characterize the clinical feature and surgical results of HOCM patients without intrinsic MV diseases undergoing mitral subvalvular procedures in addition to myectomy in comparison with those receiving myectomy alone.</p><p><strong>Methods: </strong>Among 181 eligible patients, 50 (27.6%) patients undergoing myectomy plus mitral subvalvular procedures were entered into the combined group, and the remaining 131 patients receiving myectomy alone were included in the alone group. Baseline and surgical characteristics were investigated, and surgical results were compared.</p><p><strong>Results: </strong>Comparatively, the combined group was younger (52.9 ± 11.2 years vs. 56.8 ± 11.8 years, <i>p</i>=0.045) and had a better New York Heart Association (NYHA) class (<i>p</i>=0.034) and less septal hypertrophy (16.4 ± 2.3 mm vs. 18.5 ± 3.2 mm, <i>p</i> < 0.001). Septal thickness was independently associated with combined procedures in multivariable logistic regression analysis (OR = 0.887, 95% CI 0.612-0.917). No surgical death or iatrogenic septal perforation occurred in the combined group. Two (6.5%) patients in the combined group developed complete atrioventricular block and required permanent pacemaker implantation. During a median follow-up of 10 months, no deaths or reoperations were observed with the symptom of relief and NYHA class I or II in either group. Patients in the combined group as compared to the alone group had lower outflow tract gradients and a lower incidence of residual systolic anterior motion (SAM) syndrome.</p><p><strong>Conclusions: </strong>For HOCM patients without intrinsic MV diseases who are scheduled for surgery, a less pronounced septal hypertrophy may be closely associated with myectomy with concomitant mitral subvalvular procedures instead of myectomy alone. Mitral subvalvular procedures during myectomy are safe and allow the reduction of outflow tract gradients and freedom from SAM more effectively in comparison with myectomy alone.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2020 ","pages":"8875405"},"PeriodicalIF":1.8000,"publicationDate":"2020-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7744219/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2020/8875405","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Mitral subvalvular procedures have acquired a major role during hypertrophic obstructive cardiomyopathy (HOCM) surgery. However, few studies have focused on characterizing the clinical feature of HOCM patients without intrinsic mitral valve (MV) diseases undergoing mitral subvalvular procedures in addition to myectomy. Additionally, scant data about the results of mitral subvalvular procedures during HOCM surgery are available. This single-center study aims to characterize the clinical feature and surgical results of HOCM patients without intrinsic MV diseases undergoing mitral subvalvular procedures in addition to myectomy in comparison with those receiving myectomy alone.
Methods: Among 181 eligible patients, 50 (27.6%) patients undergoing myectomy plus mitral subvalvular procedures were entered into the combined group, and the remaining 131 patients receiving myectomy alone were included in the alone group. Baseline and surgical characteristics were investigated, and surgical results were compared.
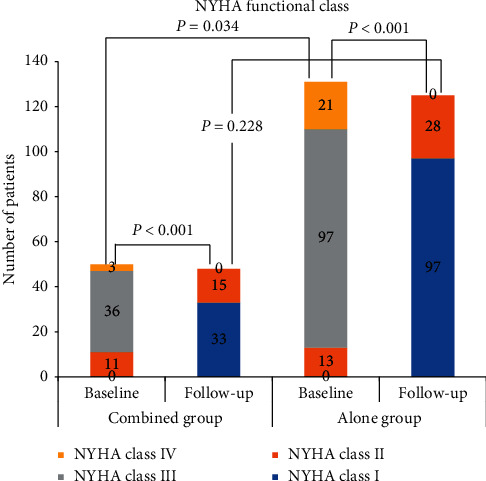
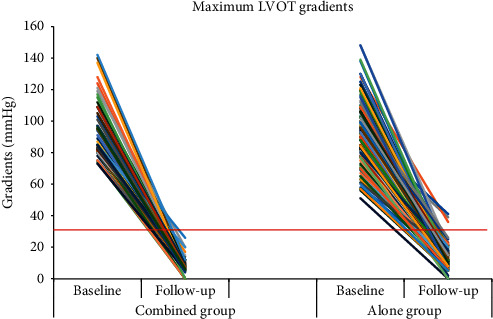
Results: Comparatively, the combined group was younger (52.9 ± 11.2 years vs. 56.8 ± 11.8 years, p=0.045) and had a better New York Heart Association (NYHA) class (p=0.034) and less septal hypertrophy (16.4 ± 2.3 mm vs. 18.5 ± 3.2 mm, p < 0.001). Septal thickness was independently associated with combined procedures in multivariable logistic regression analysis (OR = 0.887, 95% CI 0.612-0.917). No surgical death or iatrogenic septal perforation occurred in the combined group. Two (6.5%) patients in the combined group developed complete atrioventricular block and required permanent pacemaker implantation. During a median follow-up of 10 months, no deaths or reoperations were observed with the symptom of relief and NYHA class I or II in either group. Patients in the combined group as compared to the alone group had lower outflow tract gradients and a lower incidence of residual systolic anterior motion (SAM) syndrome.
Conclusions: For HOCM patients without intrinsic MV diseases who are scheduled for surgery, a less pronounced septal hypertrophy may be closely associated with myectomy with concomitant mitral subvalvular procedures instead of myectomy alone. Mitral subvalvular procedures during myectomy are safe and allow the reduction of outflow tract gradients and freedom from SAM more effectively in comparison with myectomy alone.
背景:二尖瓣瓣下手术在肥厚性梗阻性心肌病(HOCM)手术中起着重要作用。然而,很少有研究关注没有内源性二尖瓣(MV)疾病的HOCM患者在接受二尖瓣下手术和心肌切除术后的临床特征。此外,关于HOCM手术中二尖瓣下手术结果的数据很少。本单中心研究的目的是比较无内源性中压疾病的HOCM患者在二尖瓣下行二尖瓣下切除与单纯行二尖瓣下切除的临床特征和手术结果。方法:在181例符合条件的患者中,50例(27.6%)行心肌切除术加二尖瓣下手术的患者被纳入联合组,其余131例仅行心肌切除术的患者被纳入单独组。调查基线和手术特征,并比较手术结果。结果:与对照组相比,联合组更年轻(52.9±11.2岁比56.8±11.8岁,p=0.045),纽约心脏协会(NYHA)分级更优(p=0.034),室间隔肥厚更少(16.4±2.3 mm比18.5±3.2 mm, p < 0.001)。在多变量logistic回归分析中,间隔厚度与联合手术独立相关(OR = 0.887, 95% CI 0.612-0.917)。联合组无手术死亡或医源性室间隔穿孔发生。联合组2例(6.5%)患者出现完全性房室传导阻滞,需要植入永久性起搏器。在中位随访10个月期间,两组均未观察到症状缓解和NYHA I级或II级的死亡或再手术。与单独用药组相比,联合用药组患者流出道梯度较低,残余收缩前运动(SAM)综合征发生率较低。结论:对于没有内源性中枢性疾病且计划手术的HOCM患者,较不明显的室间隔肥厚可能与肌切除术合并二尖瓣下手术密切相关,而不是单纯的肌切除术。与单纯的心肌切除术相比,二尖瓣下手术是安全的,可以减少流出道梯度,更有效地避免SAM。
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
