Dustin Baldwin, Lisa Sanchez-Johnsen, Roberto Bustos, Alberto Mangano, Mario Masrur
{"title":"Metabolic Surgery Outcomes in U.S. Patients with Class I Obesity.","authors":"Dustin Baldwin, Lisa Sanchez-Johnsen, Roberto Bustos, Alberto Mangano, Mario Masrur","doi":"10.1089/bari.2020.0046","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Background:</i></b> Although numerous studies outside the United States (U.S.) have explored weight loss and comorbidity resolution among patients with class I obesity (body mass index [BMI] 30-34.9 kg/m<sup>2</sup>) after metabolic surgery, few U.S.-based studies have been conducted. <b><i>Objective:</i></b> Our aim was to compare weight loss and comorbidity resolution among U.S. patients with class I obesity, who underwent laparoscopic sleeve gastrectomy (LSG) versus Roux-en-Y gastric bypass (RYGB). <b><i>Methods:</i></b> Weight loss and comorbidity data among only patients with class I obesity, who underwent LSG or RYGB, were examined. Between April 2009 and April 2017, 1215 metabolic surgeries were performed with 30 patients meeting the inclusion criteria (17 LSG and 13 RYGB). <b><i>Results:</i></b> Percent total weight loss (%TWL) for LSG peaked at 12 months (20.85%), while RYGB %TWL peaked at 18 months (21.65%). Percent excess weight loss (%EWL) peaked at 12 months after LSG (83.59%) and 18 months after RYGB (98.29%). Overall follow-up was 56.3%, 36.7%, and 43.3% at 12, 18, and 24 months. LSG and RYGB were both successful with regard to resolution of medical comorbidities at 12 months. <b><i>Conclusion:</i></b> RYGB and LSG appear to have similar, successful outcomes among U.S. patients with class I obesity for weight loss and comorbidity resolution.</p>","PeriodicalId":48848,"journal":{"name":"Bariatric Surgical Practice and Patient Care","volume":"16 2","pages":"85-91"},"PeriodicalIF":0.3000,"publicationDate":"2021-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8217597/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bariatric Surgical Practice and Patient Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1089/bari.2020.0046","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/6/10 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 3
Abstract
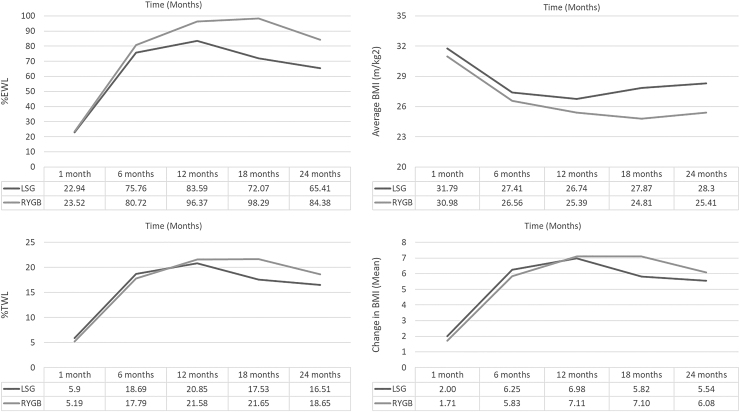
Background: Although numerous studies outside the United States (U.S.) have explored weight loss and comorbidity resolution among patients with class I obesity (body mass index [BMI] 30-34.9 kg/m2) after metabolic surgery, few U.S.-based studies have been conducted. Objective: Our aim was to compare weight loss and comorbidity resolution among U.S. patients with class I obesity, who underwent laparoscopic sleeve gastrectomy (LSG) versus Roux-en-Y gastric bypass (RYGB). Methods: Weight loss and comorbidity data among only patients with class I obesity, who underwent LSG or RYGB, were examined. Between April 2009 and April 2017, 1215 metabolic surgeries were performed with 30 patients meeting the inclusion criteria (17 LSG and 13 RYGB). Results: Percent total weight loss (%TWL) for LSG peaked at 12 months (20.85%), while RYGB %TWL peaked at 18 months (21.65%). Percent excess weight loss (%EWL) peaked at 12 months after LSG (83.59%) and 18 months after RYGB (98.29%). Overall follow-up was 56.3%, 36.7%, and 43.3% at 12, 18, and 24 months. LSG and RYGB were both successful with regard to resolution of medical comorbidities at 12 months. Conclusion: RYGB and LSG appear to have similar, successful outcomes among U.S. patients with class I obesity for weight loss and comorbidity resolution.
期刊介绍:
Bariatric Surgical Practice and Patient Care is the essential peer-reviewed journal delivering clinical best practices and quality updates for achieving optimal bariatric surgical outcomes.
Bariatric Surgical Practice and Patient Care coverage includes:
Quality outcomes measurement and reporting
Process innovations and care delivery
Short- and long-term surgical complications
Pre-surgical diagnosis and consultation
Pre-op, peri-op, and post-op standards of practice
Patient access
Patient safety issues
Nutritional and dietary support
Bariatric surgical emergencies
Best practices and current standards for bariatric surgery
Culture and ethics
Body contouring and reconstructive surgery
Bariatric teamwork and communication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
