Laureano Quintero, Juan José Meléndez-Lugo, Helmer Emilio Palacios-Rodríguez, Yaset Caicedo, Natalia Padilla, Linda M Gallego, Luis Fernando Pino, Alberto García, Adolfo González-Hadad, Mario Alain Herrera, Alexander Salcedo, José Julián Serna, Fernando Rodríguez-Holguín, Michael W Parra, Carlos A Ordoñez
{"title":"Damage control in the emergency department, a bridge to life.","authors":"Laureano Quintero, Juan José Meléndez-Lugo, Helmer Emilio Palacios-Rodríguez, Yaset Caicedo, Natalia Padilla, Linda M Gallego, Luis Fernando Pino, Alberto García, Adolfo González-Hadad, Mario Alain Herrera, Alexander Salcedo, José Julián Serna, Fernando Rodríguez-Holguín, Michael W Parra, Carlos A Ordoñez","doi":"10.25100/cm.v52i2.4801","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with hemodynamic instability have a sustained systolic blood pressure less or equal to 90 mmHg, a heart rate greater or equal to 120 beats per minute and an acute compromise of the ventilation/oxygenation ratio and/or an altered state of consciousness upon admission. These patients have higher mortality rates due to massive hemorrhage, airway injury and/or impaired ventilation. Damage control resuscitation is a systematic approach that aims to limit physiologic deterioration through strategies that address the physiologic debt of trauma. This article aims to describe the experience earned by the Trauma and Emergency Surgery Group (CTE) of Cali, Colombia in the management of the severely injured trauma patient in the emergency department following the basic principles of damage control surgery. Since bleeding is the main cause of death, the management of the severely injured trauma patient in the emergency department requires a multidisciplinary team that performs damage control maneuvers aimed at rapidly controlling bleeding, hemostatic resuscitation, and/or prompt transfer to the operating room, if required.</p>","PeriodicalId":72638,"journal":{"name":"","volume":"52 2","pages":"e4004801"},"PeriodicalIF":0.0,"publicationDate":"2021-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/76/19/1657-9534-cm-52-02-e4004801.PMC8216048.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.25100/cm.v52i2.4801","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
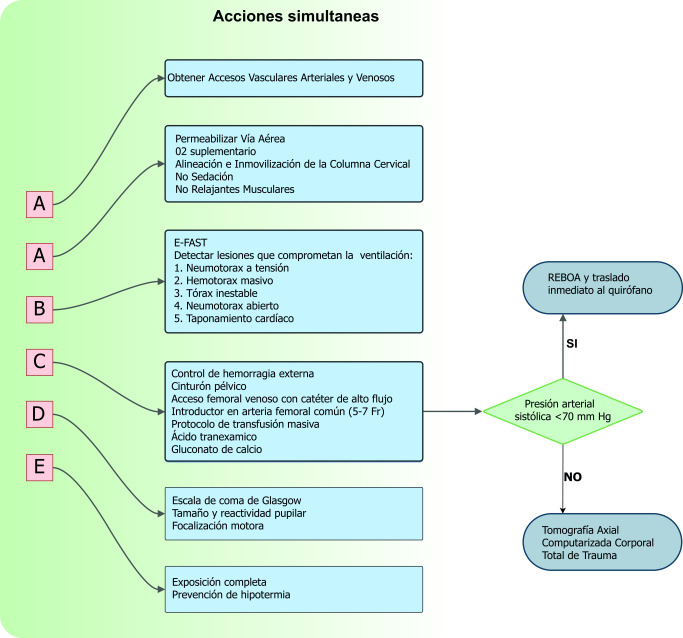
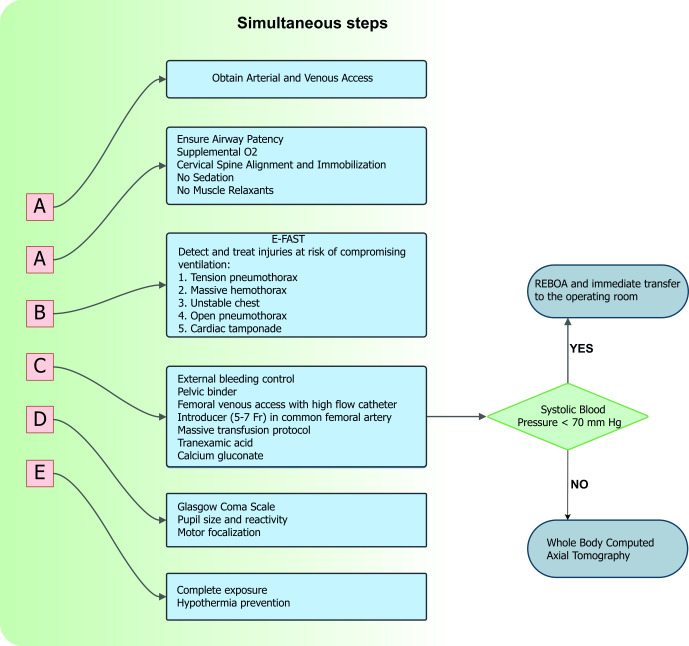
Patients with hemodynamic instability have a sustained systolic blood pressure less or equal to 90 mmHg, a heart rate greater or equal to 120 beats per minute and an acute compromise of the ventilation/oxygenation ratio and/or an altered state of consciousness upon admission. These patients have higher mortality rates due to massive hemorrhage, airway injury and/or impaired ventilation. Damage control resuscitation is a systematic approach that aims to limit physiologic deterioration through strategies that address the physiologic debt of trauma. This article aims to describe the experience earned by the Trauma and Emergency Surgery Group (CTE) of Cali, Colombia in the management of the severely injured trauma patient in the emergency department following the basic principles of damage control surgery. Since bleeding is the main cause of death, the management of the severely injured trauma patient in the emergency department requires a multidisciplinary team that performs damage control maneuvers aimed at rapidly controlling bleeding, hemostatic resuscitation, and/or prompt transfer to the operating room, if required.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
