Carole E. Aubert , Jin-Kyung Ha , Eve A. Kerr , Timothy P. Hofer , Lillian Min
{"title":"Factors associated with antihypertensive treatment intensification and deintensification in older outpatients","authors":"Carole E. Aubert , Jin-Kyung Ha , Eve A. Kerr , Timothy P. Hofer , Lillian Min","doi":"10.1016/j.ijchy.2021.100098","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>New hypertension performance measures encourage more intensive treatment in older adults. Treatment intensification includes starting new medications and increasing the dose of old ones. Medication dose is particularly important to older adults, given their vulnerability to dose-related side effects. We previously validated a standardized measure of beneficial doses tested in hypertension trials, Hypertension Daily Dose (HDD).</p></div><div><h3>Aim of the study</h3><p>To test whether changes in treatment intensity using HDD was associated with systolic blood pressure (SBP) and patient characteristics.</p></div><div><h3>Methods</h3><p>Longitudinal study of all Veterans aged ≥65 years with a diagnosis of hypertension. We defined 3 groups of risk: 1) cardiovascular risk; 2) geriatric/frail; 3) low-risk (comparator). Using multinomial regression, we assessed the probability of deintensification, intensification, vs. stable treatment, according to SBP and group.</p></div><div><h3>Results</h3><p>Among 1,331,111 Veterans, 19.9% had deintensification, and 29.6% intensification. Deintensification decreased, while intensification increased, with SBP. Compared to low-risk patients, cardiovascular risk patients had 1.11 (95% CI 1.10–1.13) times the odds of intensifying, and geriatric/frail patients 1.45 (95%CI 1.43–1.47) times the odds of deintensifying.</p></div><div><h3>Discussion</h3><p>Patient-level HDD change was consistent with an expected association with cardiovascular risk and geriatric/frail conditions, suggesting that HDD can be used longitudinally to assess hypertension treatment modification in large health systems.</p></div>","PeriodicalId":36839,"journal":{"name":"International Journal of Cardiology: Hypertension","volume":"9 ","pages":"Article 100098"},"PeriodicalIF":0.0000,"publicationDate":"2021-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchy.2021.100098","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiology: Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590086221000173","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background
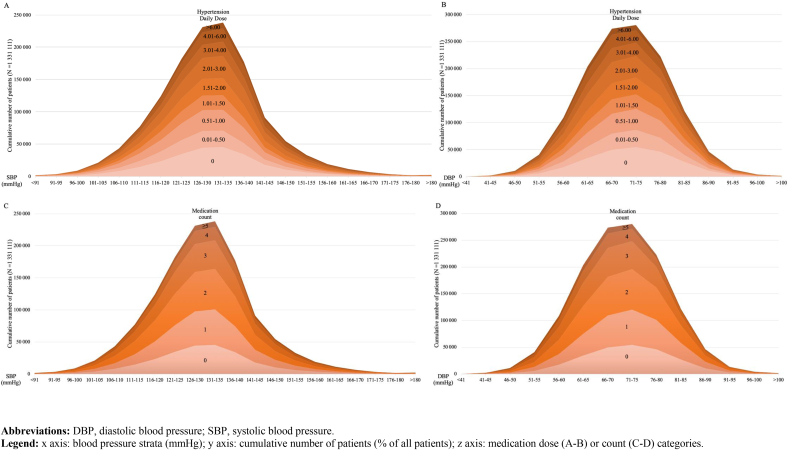
New hypertension performance measures encourage more intensive treatment in older adults. Treatment intensification includes starting new medications and increasing the dose of old ones. Medication dose is particularly important to older adults, given their vulnerability to dose-related side effects. We previously validated a standardized measure of beneficial doses tested in hypertension trials, Hypertension Daily Dose (HDD).
Aim of the study
To test whether changes in treatment intensity using HDD was associated with systolic blood pressure (SBP) and patient characteristics.
Methods
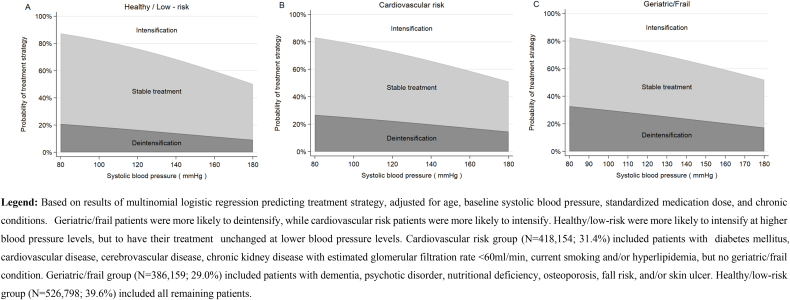
Longitudinal study of all Veterans aged ≥65 years with a diagnosis of hypertension. We defined 3 groups of risk: 1) cardiovascular risk; 2) geriatric/frail; 3) low-risk (comparator). Using multinomial regression, we assessed the probability of deintensification, intensification, vs. stable treatment, according to SBP and group.
Results
Among 1,331,111 Veterans, 19.9% had deintensification, and 29.6% intensification. Deintensification decreased, while intensification increased, with SBP. Compared to low-risk patients, cardiovascular risk patients had 1.11 (95% CI 1.10–1.13) times the odds of intensifying, and geriatric/frail patients 1.45 (95%CI 1.43–1.47) times the odds of deintensifying.
Discussion
Patient-level HDD change was consistent with an expected association with cardiovascular risk and geriatric/frail conditions, suggesting that HDD can be used longitudinally to assess hypertension treatment modification in large health systems.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
