Payal H Desai, Olesya Taylor, Kunal J Shah, Kirk E Evoy, Alyssa M Peckham
{"title":"Characterization of hospitalized patients who received naloxone while receiving opioids with or without gabapentinoids.","authors":"Payal H Desai, Olesya Taylor, Kunal J Shah, Kirk E Evoy, Alyssa M Peckham","doi":"10.9740/mhc.2021.07.225","DOIUrl":null,"url":null,"abstract":"Introduction Gabapentin and pregabalin (gabapentinoids) can be given with opioids for opioid-sparing and adjuvant analgesic effects. In the context of certain comorbidities and high dosages, coadministration of these agents can lead to respiratory depression or oversedation, necessitating naloxone administration. Methods A retrospective chart review from January 2015 to December 2017 was conducted to include patients who received naloxone and opioids with or without gabapentinoids. Exclusion criteria included pregnancy or having received naloxone in the emergency department, intensive care, or pediatrics units. The primary outcome was to characterize differences between groups regarding comorbidities, history of renal or hepatic dysfunction, history of SUD, opioid tolerance, initiation and dose appropriateness of gabapentinoids, and dose intensity of gabapentinoids and opioids. Secondary outcomes were concomitant CNS depressant use and naloxone episodes for documented respiratory depression. Results Of 126 patients who met inclusion criteria, 36 received opioids and gabapentinoids (gabapentinoid group) and 90 received opioids alone (nongabapentinoid group). There were 136 naloxone episodes between the 2 groups. More than 50% of the naloxone episodes in the gabapentinoid group involved opioids of at least 90 oral morphine mg equivalents. Respiratory depression accounted for 39% and 15.8% of the naloxone episodes in the gabapentinoid and nongabapentinoid groups, respectively. Discussion There may be increased naloxone episodes among patients receiving opioids and gabapentinoids. Future studies are needed to evaluate the incremental risk of respiratory depression and oversedation as it pertains to concomitant medication administration and patient-specific factors.","PeriodicalId":22710,"journal":{"name":"The Mental Health Clinician","volume":"11 4","pages":"225-230"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/5e/i2168-9709-11-4-225.PMC8287869.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Mental Health Clinician","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9740/mhc.2021.07.225","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
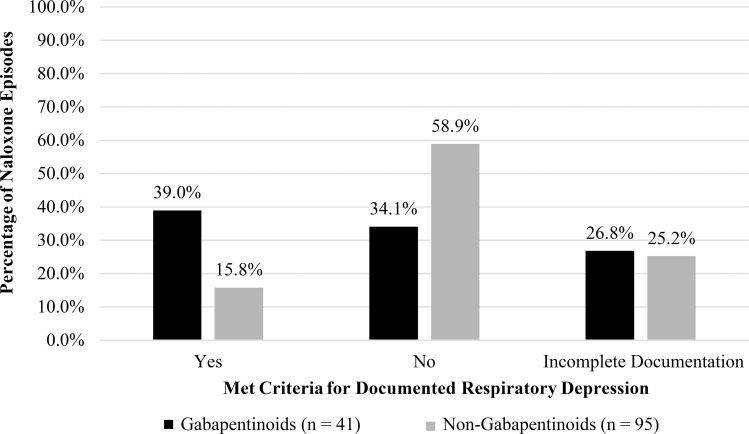
Introduction Gabapentin and pregabalin (gabapentinoids) can be given with opioids for opioid-sparing and adjuvant analgesic effects. In the context of certain comorbidities and high dosages, coadministration of these agents can lead to respiratory depression or oversedation, necessitating naloxone administration. Methods A retrospective chart review from January 2015 to December 2017 was conducted to include patients who received naloxone and opioids with or without gabapentinoids. Exclusion criteria included pregnancy or having received naloxone in the emergency department, intensive care, or pediatrics units. The primary outcome was to characterize differences between groups regarding comorbidities, history of renal or hepatic dysfunction, history of SUD, opioid tolerance, initiation and dose appropriateness of gabapentinoids, and dose intensity of gabapentinoids and opioids. Secondary outcomes were concomitant CNS depressant use and naloxone episodes for documented respiratory depression. Results Of 126 patients who met inclusion criteria, 36 received opioids and gabapentinoids (gabapentinoid group) and 90 received opioids alone (nongabapentinoid group). There were 136 naloxone episodes between the 2 groups. More than 50% of the naloxone episodes in the gabapentinoid group involved opioids of at least 90 oral morphine mg equivalents. Respiratory depression accounted for 39% and 15.8% of the naloxone episodes in the gabapentinoid and nongabapentinoid groups, respectively. Discussion There may be increased naloxone episodes among patients receiving opioids and gabapentinoids. Future studies are needed to evaluate the incremental risk of respiratory depression and oversedation as it pertains to concomitant medication administration and patient-specific factors.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
