Bibi Uhre Nielsen, Daniel Faurholt-Jepsen, Peter Sandor Oturai, Tavs Qvist, Rikke Krogh-Madsen, Terese Lea Katzenstein, James Shaw, Christian Ritz, Tacjana Pressler, Thomas Peter Almdal, Inger Hee Mabuza Mathiesen
{"title":"Associations Between Glucose Tolerance, Insulin Secretion, Muscle and Fat Mass in Cystic Fibrosis.","authors":"Bibi Uhre Nielsen, Daniel Faurholt-Jepsen, Peter Sandor Oturai, Tavs Qvist, Rikke Krogh-Madsen, Terese Lea Katzenstein, James Shaw, Christian Ritz, Tacjana Pressler, Thomas Peter Almdal, Inger Hee Mabuza Mathiesen","doi":"10.1177/11795514211038259","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A frequent comorbidity in cystic fibrosis (CF) is CF related diabetes (CFRD) caused by a gradual decline in insulin secretion. The reduction in the anabolic hormone, insulin, might explain the weight loss that precedes onset of CFRD. We investigated the association between muscle and fat mass in relation to glucose tolerance and insulin function.</p><p><strong>Methods: </strong>In a cross-sectional study with CF patients (⩾18 years), we conducted an oral glucose tolerance test and dual energy X-ray absorptiometry scan (DXA). Based on plasma glucose, glucose tolerance was defined as normal (NGT): 1-hour <11.1 mmol/L and 2-hour <7.8 mmol/L, impaired (IGT): 2-hour ⩾7.8 and <11.1 mmol/L or CFRD: 2-hour ⩾11.1 mmol/L. Insulin resistance (HOMA-IR) was derived from fasting levels of plasma glucose and plasma insulin, and fat-free and fat mass index (kg/m<sup>2</sup>) from DXA. Associations were evaluated using linear regression models adjusted for age, sex, and pancreas insufficiency.</p><p><strong>Results: </strong>Among 79 CF patients with exocrine pancreas insufficiency, impairment of glucose tolerance corresponded to reduced insulin secretion. In the IGT group the fat-free mass index (FFMI) was 1.2 kg/m<sup>2</sup> (95% CI: [-2.3, -0.03] kg/m<sup>2</sup>, <i>P</i> = .044) lower compared to the NGT group. FFMI increased insignificantly by 0.4 kg/m<sup>2</sup> (95% CI: [-0.6, 1.5] kg/m<sup>2</sup>, <i>P</i> = .422) among the insulin-treated CFRD group compared to IGT. Fat mass index (FMI) was not different between groups but tended to decrease with glucose tolerance impairment. For each 100 pmol/L increase in fasting insulin FFMI increased by 1.77 kg/m<sup>2</sup> (95% CI: [0.21, 3.33] kg/m<sup>2</sup>/pmol/L/100) and FMI increased by 6.15 kg/m<sup>2</sup> (95% CI: [3.87, 8.44] kg/m<sup>2</sup>/pmol/L/100). In multivariate analyses, HOMA-IR was positively associated with FFMI (β = 0.5 kg/m<sup>2</sup>/HOMA-IR, 95% CI: [0.08, 0.92] kg/m<sup>2</sup>/HOMA-IR, <i>P</i> = .021) and FMI (β = 1.5 kg/m<sup>2</sup>/HOMA-IR, 95% CI: [0.87, 2.15] kg/m<sup>2</sup>/HOMA-IR, <i>P</i> < .001).</p><p><strong>Conclusions: </strong>Muscle mass was significantly lower among participants with impaired glucose tolerance (IGT), while muscle mass was normalized among those treated with insulin.</p>","PeriodicalId":44715,"journal":{"name":"Clinical Medicine Insights-Endocrinology and Diabetes","volume":"14 ","pages":"11795514211038259"},"PeriodicalIF":3.0000,"publicationDate":"2021-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/4f/10.1177_11795514211038259.PMC8369959.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Endocrinology and Diabetes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795514211038259","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 4
Abstract
Background: A frequent comorbidity in cystic fibrosis (CF) is CF related diabetes (CFRD) caused by a gradual decline in insulin secretion. The reduction in the anabolic hormone, insulin, might explain the weight loss that precedes onset of CFRD. We investigated the association between muscle and fat mass in relation to glucose tolerance and insulin function.
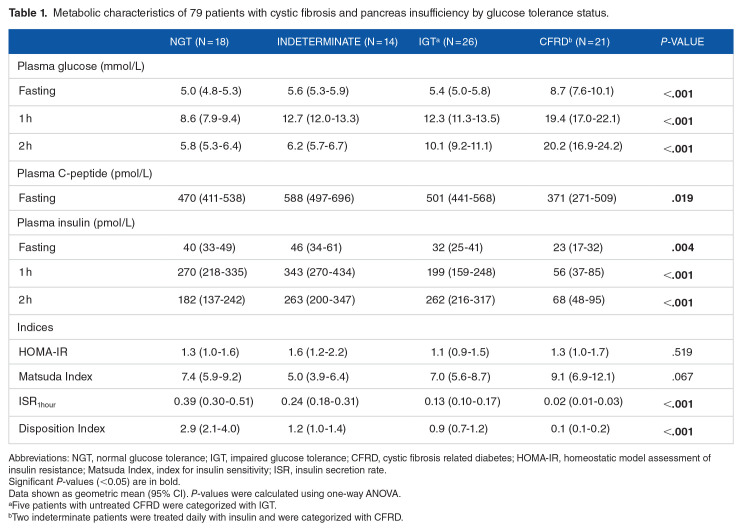
Methods: In a cross-sectional study with CF patients (⩾18 years), we conducted an oral glucose tolerance test and dual energy X-ray absorptiometry scan (DXA). Based on plasma glucose, glucose tolerance was defined as normal (NGT): 1-hour <11.1 mmol/L and 2-hour <7.8 mmol/L, impaired (IGT): 2-hour ⩾7.8 and <11.1 mmol/L or CFRD: 2-hour ⩾11.1 mmol/L. Insulin resistance (HOMA-IR) was derived from fasting levels of plasma glucose and plasma insulin, and fat-free and fat mass index (kg/m2) from DXA. Associations were evaluated using linear regression models adjusted for age, sex, and pancreas insufficiency.
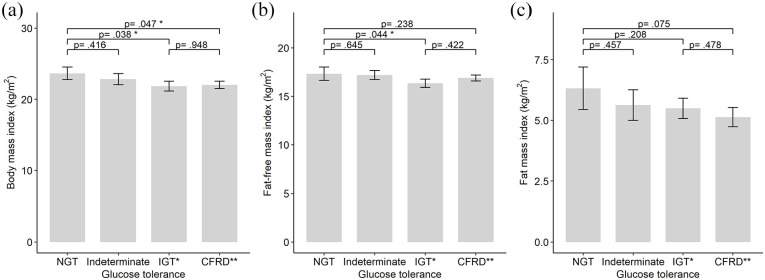
Results: Among 79 CF patients with exocrine pancreas insufficiency, impairment of glucose tolerance corresponded to reduced insulin secretion. In the IGT group the fat-free mass index (FFMI) was 1.2 kg/m2 (95% CI: [-2.3, -0.03] kg/m2, P = .044) lower compared to the NGT group. FFMI increased insignificantly by 0.4 kg/m2 (95% CI: [-0.6, 1.5] kg/m2, P = .422) among the insulin-treated CFRD group compared to IGT. Fat mass index (FMI) was not different between groups but tended to decrease with glucose tolerance impairment. For each 100 pmol/L increase in fasting insulin FFMI increased by 1.77 kg/m2 (95% CI: [0.21, 3.33] kg/m2/pmol/L/100) and FMI increased by 6.15 kg/m2 (95% CI: [3.87, 8.44] kg/m2/pmol/L/100). In multivariate analyses, HOMA-IR was positively associated with FFMI (β = 0.5 kg/m2/HOMA-IR, 95% CI: [0.08, 0.92] kg/m2/HOMA-IR, P = .021) and FMI (β = 1.5 kg/m2/HOMA-IR, 95% CI: [0.87, 2.15] kg/m2/HOMA-IR, P < .001).
Conclusions: Muscle mass was significantly lower among participants with impaired glucose tolerance (IGT), while muscle mass was normalized among those treated with insulin.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
