Maria Goretti Moreira Guimarães Penido, Marcelo de Sousa Tavares
{"title":"Should pediatric idiopathic hypercalciuria be treated with hypocalciuric agents?","authors":"Maria Goretti Moreira Guimarães Penido, Marcelo de Sousa Tavares","doi":"10.5527/wjn.v10.i4.47","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hypercalciuria is the most common metabolic risk factor for calcium urolithiasis and is associated with bone loss in adult patients. Reduced bone mineral density (BMD) was already described in idiopathic hypercalciuria (IH) children, but the precise mechanisms of bone loss or inadequate bone mass gain remain unknown. Life-long hypercalciuria might be considered a risk to change bone structure and determine low bone mass throughout life. The peak of bone mass should occur without interferences. A beneficial effect of citrate formulations and thiazides on bone mass in adult and pediatric patients with IH have been shown.</p><p><strong>Aim: </strong>To evaluate whether pharmacological therapy has a beneficial effect on bone mass in children and adolescents with IH.</p><p><strong>Methods: </strong>This retrospective cohort study evaluated 40 hypercalciuric children non-responsive to lifestyle and diet changes. After a 2-mo run-in period of citrate formulation (Kcitrate) usage, the first bone densitometry (DXA) was ordered. In patients with sustained hypercalciuria, a thiazide diuretic was prescribed. The second DXA was performed after 12 mo. Bone densitometry was performed by DXA at lumbar spine (L2-L4). A 24-h urine (calcium, citrate, creatinine) and blood samples (urea, creatinine, uric acid, calcium, phosphorus, magnesium, chloride, hemoglobin) were obtained. Clinical data included age, gender, weight, height and body mass index.</p><p><strong>Results: </strong>Forty IH children; median age 10.5 year and median time follow-up 6.0 year were evaluated. Nine patients were treated with Kcitrate (G1) and 31 with Kcitrate + thiazide (G2). There were no differences in age, gender, body mass index <i>z</i>-score and biochemical parameters between G1 and G2. There were no increases in total cholesterol, kalemia and magnesemia. Calciuria decreased in both groups after treatment. Lumbar spine BMD <i>z</i>-score increased after thiazide treatment in G2. There was no improvement in G1.</p><p><strong>Conclusion: </strong>Results point to a beneficial effect of thiazide on lumbar spine BMD <i>z</i>-score in children with IH. Further studies are necessary to confirm the results of the present study.</p>","PeriodicalId":23745,"journal":{"name":"World Journal of Nephrology","volume":"10 4","pages":"47-58"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/ae/WJN-10-47.PMC8353600.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v10.i4.47","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Hypercalciuria is the most common metabolic risk factor for calcium urolithiasis and is associated with bone loss in adult patients. Reduced bone mineral density (BMD) was already described in idiopathic hypercalciuria (IH) children, but the precise mechanisms of bone loss or inadequate bone mass gain remain unknown. Life-long hypercalciuria might be considered a risk to change bone structure and determine low bone mass throughout life. The peak of bone mass should occur without interferences. A beneficial effect of citrate formulations and thiazides on bone mass in adult and pediatric patients with IH have been shown.
Aim: To evaluate whether pharmacological therapy has a beneficial effect on bone mass in children and adolescents with IH.
Methods: This retrospective cohort study evaluated 40 hypercalciuric children non-responsive to lifestyle and diet changes. After a 2-mo run-in period of citrate formulation (Kcitrate) usage, the first bone densitometry (DXA) was ordered. In patients with sustained hypercalciuria, a thiazide diuretic was prescribed. The second DXA was performed after 12 mo. Bone densitometry was performed by DXA at lumbar spine (L2-L4). A 24-h urine (calcium, citrate, creatinine) and blood samples (urea, creatinine, uric acid, calcium, phosphorus, magnesium, chloride, hemoglobin) were obtained. Clinical data included age, gender, weight, height and body mass index.
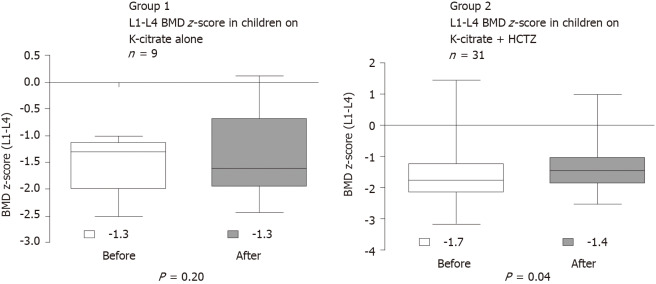
Results: Forty IH children; median age 10.5 year and median time follow-up 6.0 year were evaluated. Nine patients were treated with Kcitrate (G1) and 31 with Kcitrate + thiazide (G2). There were no differences in age, gender, body mass index z-score and biochemical parameters between G1 and G2. There were no increases in total cholesterol, kalemia and magnesemia. Calciuria decreased in both groups after treatment. Lumbar spine BMD z-score increased after thiazide treatment in G2. There was no improvement in G1.
Conclusion: Results point to a beneficial effect of thiazide on lumbar spine BMD z-score in children with IH. Further studies are necessary to confirm the results of the present study.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
