Drew Lansdown, Edward C Cheung, Weiyuan Xiao, Austin Lee, Alan L Zhang, Brian T Feeley, C Benjamin Ma
{"title":"Do Preoperative and Postoperative Glenoid Retroversion Influence Outcomes After Reverse Total Shoulder Arthroplasty?","authors":"Drew Lansdown, Edward C Cheung, Weiyuan Xiao, Austin Lee, Alan L Zhang, Brian T Feeley, C Benjamin Ma","doi":"10.1177/2471549220912552","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are limited data on the effect of glenoid retroversion in clinical outcomes following reverse total shoulder arthroplasty (RTSA). The purpose of this study was to evaluate if surgical correction of retroversion affects outcomes following RTSA.</p><p><strong>Methods: </strong>An institutional database was utilized to identify 177 patients (mean age: 68.2 ± 10.1 years) with minimum 2-year follow-up after primary RTSA. Glenoid version was measured on preoperative and postoperative radiographs. American Shoulder and Elbow Surgeons (ASES) scores and range of motion were collected before and after RTSA. Change in retroversion was determined by comparing preoperative and postoperative glenoid retroversion on radiographs using paired Wilcoxon signed-rank test. Spearman's rank correlation was used to investigate relationships between ASES scores and glenoid retroversion.</p><p><strong>Results: </strong>The mean postoperative ASES composite score (75.5 ± 22.7) was significantly higher than preoperative (36.8 ± 19.2; <i>P</i> < .0001). The mean preoperative glenoid retroversion was 9.1 ± 6.7° compared to 6.5 ± 5.1° postoperatively (<i>P</i> < .0001). There was no correlation between postoperative ASES scores and preoperative retroversion (<i>r</i> = .014, <i>P</i> = .85) or postoperative retroversion (<i>r</i> = -.043, <i>P</i> = .57). There was no statistical relationship between postoperative retroversion and range of motion, though there is a risk of inadequate power given the sample size.</p><p><strong>Conclusions: </strong>Patient-reported outcomes and range of motion measurements following RTSA at short-term follow-up appear to be independent of either preoperative or postoperative glenoid retroversion.</p>","PeriodicalId":73942,"journal":{"name":"Journal of shoulder and elbow arthroplasty","volume":"4 ","pages":"2471549220912552"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2471549220912552","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of shoulder and elbow arthroplasty","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2471549220912552","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: There are limited data on the effect of glenoid retroversion in clinical outcomes following reverse total shoulder arthroplasty (RTSA). The purpose of this study was to evaluate if surgical correction of retroversion affects outcomes following RTSA.
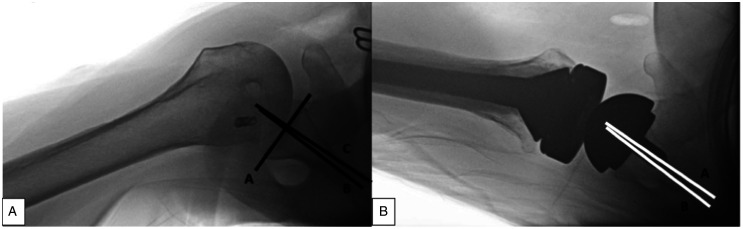
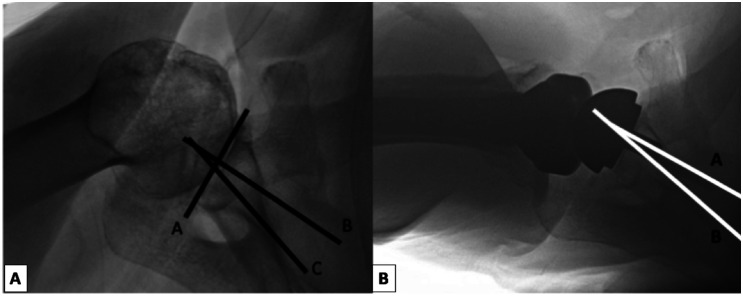
Methods: An institutional database was utilized to identify 177 patients (mean age: 68.2 ± 10.1 years) with minimum 2-year follow-up after primary RTSA. Glenoid version was measured on preoperative and postoperative radiographs. American Shoulder and Elbow Surgeons (ASES) scores and range of motion were collected before and after RTSA. Change in retroversion was determined by comparing preoperative and postoperative glenoid retroversion on radiographs using paired Wilcoxon signed-rank test. Spearman's rank correlation was used to investigate relationships between ASES scores and glenoid retroversion.
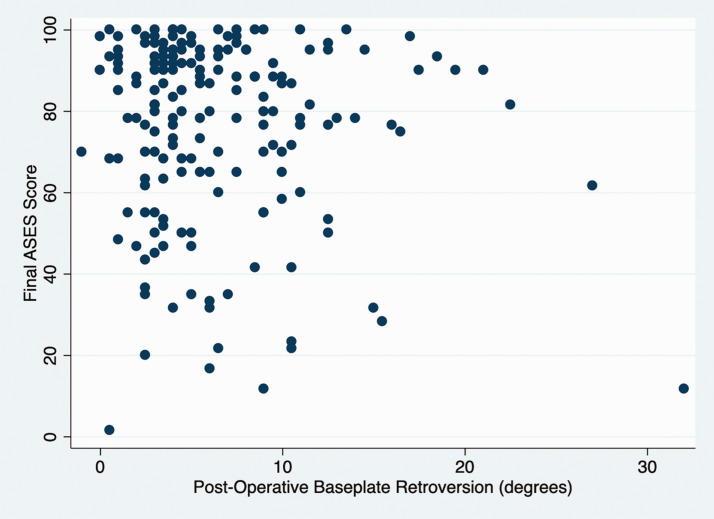
Results: The mean postoperative ASES composite score (75.5 ± 22.7) was significantly higher than preoperative (36.8 ± 19.2; P < .0001). The mean preoperative glenoid retroversion was 9.1 ± 6.7° compared to 6.5 ± 5.1° postoperatively (P < .0001). There was no correlation between postoperative ASES scores and preoperative retroversion (r = .014, P = .85) or postoperative retroversion (r = -.043, P = .57). There was no statistical relationship between postoperative retroversion and range of motion, though there is a risk of inadequate power given the sample size.
Conclusions: Patient-reported outcomes and range of motion measurements following RTSA at short-term follow-up appear to be independent of either preoperative or postoperative glenoid retroversion.
背景:关于肩胛盂后移对逆行全肩关节置换术(RTSA)后临床结果的影响的数据有限。本研究的目的是评估手术矫正后侧翻是否会影响RTSA后的预后。方法:利用机构数据库确定177例患者(平均年龄:68.2±10.1岁),首次RTSA后至少随访2年。在术前和术后x线片上测量关节盂变形。在RTSA前后收集美国肩关节外科医生(American Shoulder and肘外科医生)评分和活动范围。通过配对Wilcoxon sign -rank检验比较术前和术后x线片上关节盂后倾的变化来确定。使用Spearman等级相关来研究asas评分与关节盂后翻之间的关系。结果:术后平均as综合评分(75.5±22.7)明显高于术前(36.8±19.2);P P r =。014, P = .85)或术后逆行(r = -。043, p = .57)。虽然考虑到样本量存在功率不足的风险,但术后退位和关节活动度之间没有统计学上的关系。结论:患者报告的结果和短期随访RTSA后的活动范围测量似乎与术前或术后肩关节后翻无关。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
