S Biuden, K Maatallah, H Riahi, H Ferjani, M D Kaffel, W Hamdi
{"title":"SAPHO Syndrome Mimicking Infectious Spondylodiscitis and Bone Metastasis.","authors":"S Biuden, K Maatallah, H Riahi, H Ferjani, M D Kaffel, W Hamdi","doi":"10.1155/2021/5577257","DOIUrl":null,"url":null,"abstract":"<p><p>The acronym SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) includes diseases with similar osteoarticular manifestations and skin conditions. Making this diagnosis is not always obvious, especially when the clinical presentation does not fit the typical pattern of the disease or it occurs in a particular field. We described three cases where the diagnosis was difficult. A 46 year-old woman presented with cervical pain. The cervical X-ray showed the aspect of an ivory C5 vertebra. The patient had, however, preserved general condition, no signs of underlying neoplasia, nor other joint complaints. Blood analysis was normal. Tomography did not find any suspect lesion but showed sclerosis and hyperostosis of the manubrium. Scintigraphy showed the characteristic \"bullhead\" appearance. A 61-year-old woman had thoracic and lumbar pain. MRI showed spondylodiscitis in D3-D4, D4-D5, D5-D6, D6-D7, and L1-L2 with paraspinal soft tissue involvement, simulating infectious spondylodiscitis. Infectious investigations and discovertebral biopsy performed twice were negative. SAPHO syndrome was then suspected. Bone scintigraphy showed uptake in the chondrosternal articulations and D4 to D7 vertebrae. The diagnosis of SAPHO was established. The third case was a 46-year-old man with a lung adenocarcinoma. Staging for metastatic disease, a TAP tomography was performed and showed osteosclerosis of D8 to D12 and intra-articular bridges in the sacroiliac joints. MRI and scintigraphy eliminated malignancy and confirmed the diagnosis of SAPHO. In our cases, imaging findings could facilitate differentiating SAPHO syndrome from other diseases.</p>","PeriodicalId":9622,"journal":{"name":"Case Reports in Rheumatology","volume":"2021 ","pages":"5577257"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8437625/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5577257","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
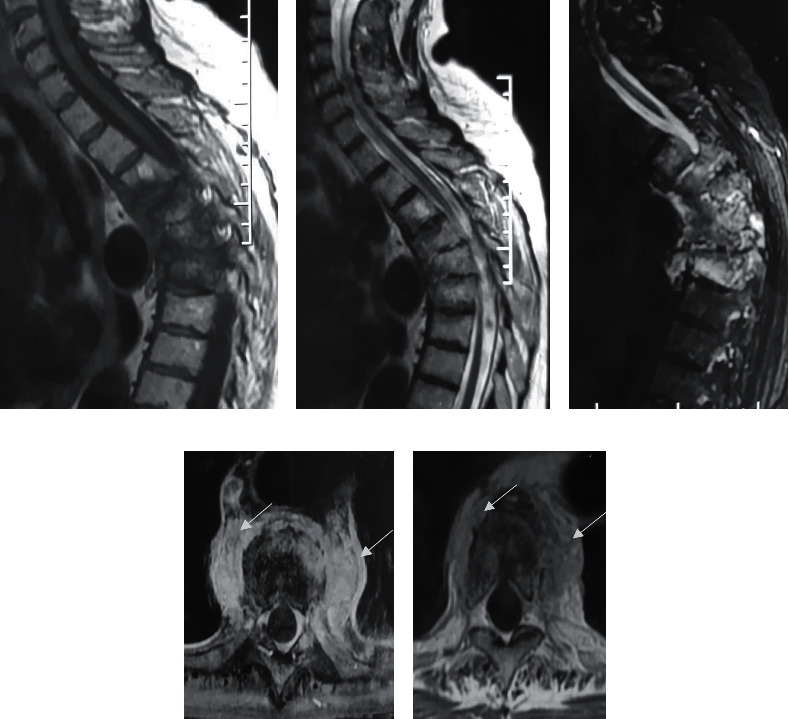
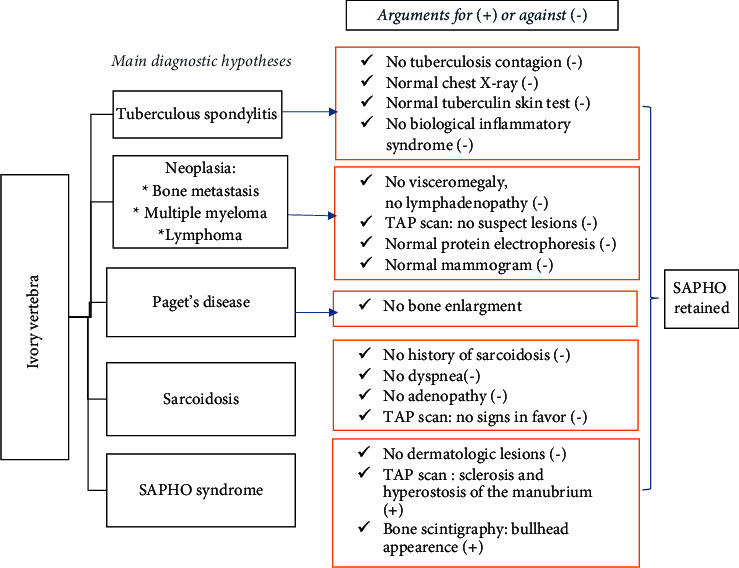
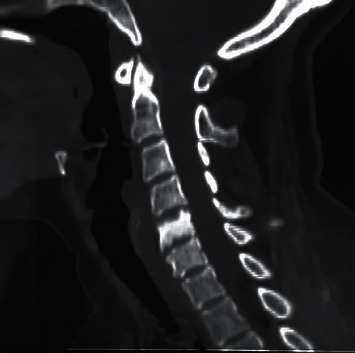
The acronym SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) includes diseases with similar osteoarticular manifestations and skin conditions. Making this diagnosis is not always obvious, especially when the clinical presentation does not fit the typical pattern of the disease or it occurs in a particular field. We described three cases where the diagnosis was difficult. A 46 year-old woman presented with cervical pain. The cervical X-ray showed the aspect of an ivory C5 vertebra. The patient had, however, preserved general condition, no signs of underlying neoplasia, nor other joint complaints. Blood analysis was normal. Tomography did not find any suspect lesion but showed sclerosis and hyperostosis of the manubrium. Scintigraphy showed the characteristic "bullhead" appearance. A 61-year-old woman had thoracic and lumbar pain. MRI showed spondylodiscitis in D3-D4, D4-D5, D5-D6, D6-D7, and L1-L2 with paraspinal soft tissue involvement, simulating infectious spondylodiscitis. Infectious investigations and discovertebral biopsy performed twice were negative. SAPHO syndrome was then suspected. Bone scintigraphy showed uptake in the chondrosternal articulations and D4 to D7 vertebrae. The diagnosis of SAPHO was established. The third case was a 46-year-old man with a lung adenocarcinoma. Staging for metastatic disease, a TAP tomography was performed and showed osteosclerosis of D8 to D12 and intra-articular bridges in the sacroiliac joints. MRI and scintigraphy eliminated malignancy and confirmed the diagnosis of SAPHO. In our cases, imaging findings could facilitate differentiating SAPHO syndrome from other diseases.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
