{"title":"Uterocutaneous Fistula after a C-Section in a Patient with Second Trimester Fetal Demise and Chorioamnionitis.","authors":"Déborah Wernly, Valérie Besse, Daniela Huber","doi":"10.1155/2021/3255188","DOIUrl":null,"url":null,"abstract":"<p><p>Uterocutaneous fistulae are very rare entities with only about 120 cases reported in the literature. They are mostly described after a C-section or other pelvic surgery. We hereby describe a uterocutaneous fistula in a 41-year-old patient 5 months after a C-section because of a chorioamnionitis and a 22-week fetal demise. One month after the C-section, she underwent a diagnostic hysteroscopy to exclude postoperative intrauterine adhesions. Afterwards, she complained of pelvic pain, persistent metrorrhagia, and significant weight loss during 2 months. She consulted the emergency unit several times, and lastly endometritis was diagnosed. She was treated with antibiotic therapy for 7 days, without significant clinical improvement. She presented at our institution 48 hours after a carbuncle had appeared in her right iliac fossa. A uterocutaneous fistula was diagnosed on the CT scan. The patient received IV antibiotic therapy and underwent a total hysterectomy with bilateral salpingectomy by laparotomy, as she did not want a conservative surgery. The clinical postoperative evolution was favorable. Symptoms of UCF can be very unspecific. To avoid medical wandering and improve the patient's care, UCF should be in the differential diagnostic of abdominal pain after a pelvic surgery. Moreover, in patients with previous C-section and infectious perioperative status, the risk of PID or pelvic abscess must be careful evaluated before intrauterine diagnostic or therapeutic procedures.</p>","PeriodicalId":9610,"journal":{"name":"Case Reports in Obstetrics and Gynecology","volume":"2021 ","pages":"3255188"},"PeriodicalIF":0.8000,"publicationDate":"2021-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8449720/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/3255188","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
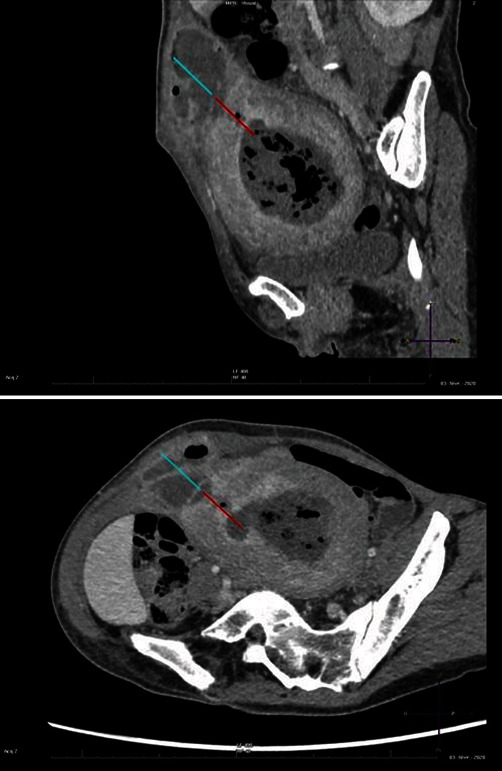
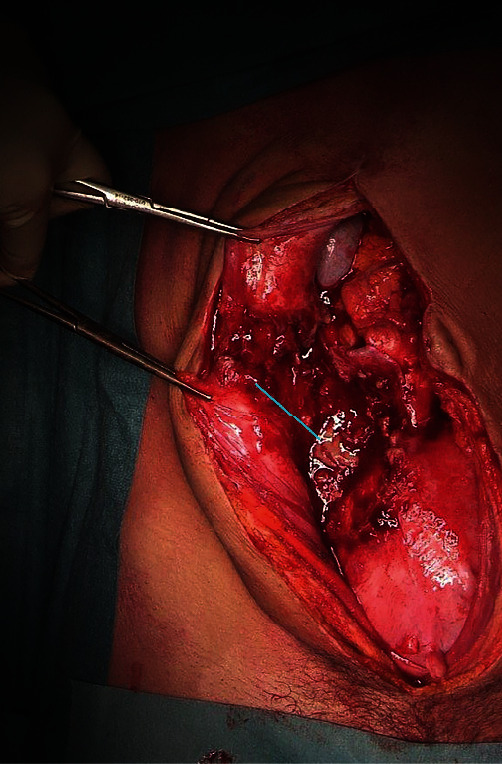
Uterocutaneous fistulae are very rare entities with only about 120 cases reported in the literature. They are mostly described after a C-section or other pelvic surgery. We hereby describe a uterocutaneous fistula in a 41-year-old patient 5 months after a C-section because of a chorioamnionitis and a 22-week fetal demise. One month after the C-section, she underwent a diagnostic hysteroscopy to exclude postoperative intrauterine adhesions. Afterwards, she complained of pelvic pain, persistent metrorrhagia, and significant weight loss during 2 months. She consulted the emergency unit several times, and lastly endometritis was diagnosed. She was treated with antibiotic therapy for 7 days, without significant clinical improvement. She presented at our institution 48 hours after a carbuncle had appeared in her right iliac fossa. A uterocutaneous fistula was diagnosed on the CT scan. The patient received IV antibiotic therapy and underwent a total hysterectomy with bilateral salpingectomy by laparotomy, as she did not want a conservative surgery. The clinical postoperative evolution was favorable. Symptoms of UCF can be very unspecific. To avoid medical wandering and improve the patient's care, UCF should be in the differential diagnostic of abdominal pain after a pelvic surgery. Moreover, in patients with previous C-section and infectious perioperative status, the risk of PID or pelvic abscess must be careful evaluated before intrauterine diagnostic or therapeutic procedures.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
