{"title":"Eosinophilic Granulomatosis Polyangiitis (EGPA) Masquerading as a Mycotic Aneurysm of the Abdominal Aorta: Case Report and Review of Literature.","authors":"Pooja Kumari, Debendra Pattanaik, Claire Williamson","doi":"10.1155/2021/7093607","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Aortic involvement leading to aortitis in eosinophilic granulomatosis polyangiitis (EGPA) is infrequent, and only 2 cases have been reported so far in the literature. Even more so, aortic aneurysm, secondary to EGPA, has never been reported and remains a diagnostic and therapeutic challenge. <i>Case Presentation</i>. We present a 63-year-old Caucasian male patient with a prior diagnosis of EGPA presenting with abdominal pain, nausea, and loose stools to the emergency department. Physical examination showed periumbilical tenderness. He had no peripheral eosinophilia but had high C-reactive protein and procalcitonin levels. CT abdomen revealed a mycotic aneurysm involving the infrarenal abdominal aorta. The patient declined surgical repair initially and was treated with IV antibiotics only. Unfortunately, 24 hours later, the aneurysm ruptured, leading to emergent axillofemoral bypass surgery. Surgical biopsy showed aortitis, periaortitis, and active necrotizing vasculitis.</p><p><strong>Conclusion: </strong>Abdominal aneurysms should be considered a complication of EGPA, and earlier immunosuppressive therapy should be considered to prevent further complications.</p>","PeriodicalId":9622,"journal":{"name":"Case Reports in Rheumatology","volume":"2021 ","pages":"7093607"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8452388/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/7093607","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
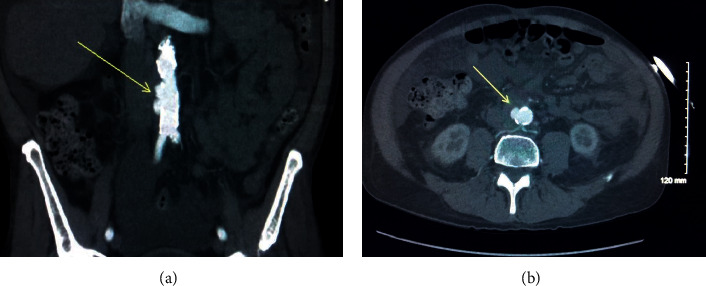
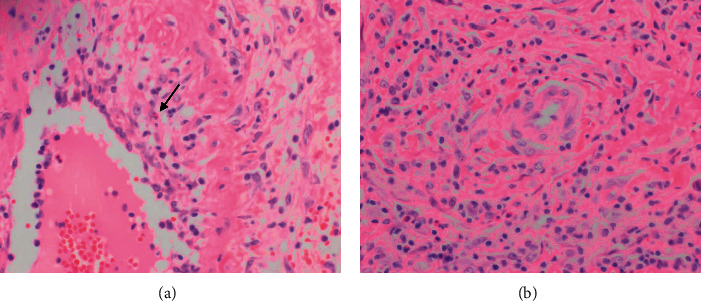
Introduction: Aortic involvement leading to aortitis in eosinophilic granulomatosis polyangiitis (EGPA) is infrequent, and only 2 cases have been reported so far in the literature. Even more so, aortic aneurysm, secondary to EGPA, has never been reported and remains a diagnostic and therapeutic challenge. Case Presentation. We present a 63-year-old Caucasian male patient with a prior diagnosis of EGPA presenting with abdominal pain, nausea, and loose stools to the emergency department. Physical examination showed periumbilical tenderness. He had no peripheral eosinophilia but had high C-reactive protein and procalcitonin levels. CT abdomen revealed a mycotic aneurysm involving the infrarenal abdominal aorta. The patient declined surgical repair initially and was treated with IV antibiotics only. Unfortunately, 24 hours later, the aneurysm ruptured, leading to emergent axillofemoral bypass surgery. Surgical biopsy showed aortitis, periaortitis, and active necrotizing vasculitis.
Conclusion: Abdominal aneurysms should be considered a complication of EGPA, and earlier immunosuppressive therapy should be considered to prevent further complications.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
