{"title":"The Feasibility of Mechanical Thrombectomy on Single-Plane Angiosuite: An In-Depth Analysis of Procedure Time.","authors":"Hiroyasu Inoue, Masahiro Oomura, Yusuke Nishikawa, Mitsuhito Mase, Noriyuki Matsukawa","doi":"10.1159/000519555","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Mechanical thrombectomy (MT) is usually performed on biplane (BP) angiosuites. When the BP angiosuite is not available, the single-plane (SP) angiosuite may be a substitute. However, the feasibility of MT performed on the SP angiosuite is yet to be elucidated. Therefore, we investigated the alternative effect of the SP angiosuite on the detailed division of procedure time, recanalization rate, and outcome in patients with anterior circulation infarction.</p><p><strong>Methods: </strong>The subjects included 80 consecutive patients with anterior circulation infarction who underwent MT at our hospital between May 2015 and December 2020. Demographics and characteristics of the BP and SP groups were assessed and compared. The time from puncture to guiding catheter placement (P-G), time from guiding catheter placement to recanalization (G-R), and time from puncture to recanalization (P-R) were also extracted. A good outcome was defined as a modified Rankin scale score ≤2 at 3 months.</p><p><strong>Results: </strong>Of the 80 patients, 67 and 13 were treated with BP and SP angiosuites, respectively. There were no differences in age, sex, complications, Alberta Stroke Program Early CT Score, National Institutes of Health Stroke Scale score at onset, occlusion site, rate of recombinant tissue-type plasminogen activator administration, stroke subtype, recanalization rate, and complications between the 2 groups. The rate of a good outcome was not different between the 2 groups. P-G was significantly longer in the SP group than in the BP group, whereas there was no significant difference in G-R and P-R between the 2 groups (P-G: BP 29.9 ± 21.8 vs. SP 48.5 ± 43.6 min, p = 0.04).</p><p><strong>Conclusion: </strong>MT performed on the SP angiosuite tended to prolong the time for guiding catheter placement. However, there was no difference in the overall procedure time, recanalization rate, or outcome between BP and SP angiosuites. Therefore, if the BP angiosuite is not available, the use of the SP angiosuite should be encouraged.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":"11 3","pages":"112-117"},"PeriodicalIF":2.1000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/35/cd/cee-0011-0112.PMC8613560.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000519555","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Mechanical thrombectomy (MT) is usually performed on biplane (BP) angiosuites. When the BP angiosuite is not available, the single-plane (SP) angiosuite may be a substitute. However, the feasibility of MT performed on the SP angiosuite is yet to be elucidated. Therefore, we investigated the alternative effect of the SP angiosuite on the detailed division of procedure time, recanalization rate, and outcome in patients with anterior circulation infarction.
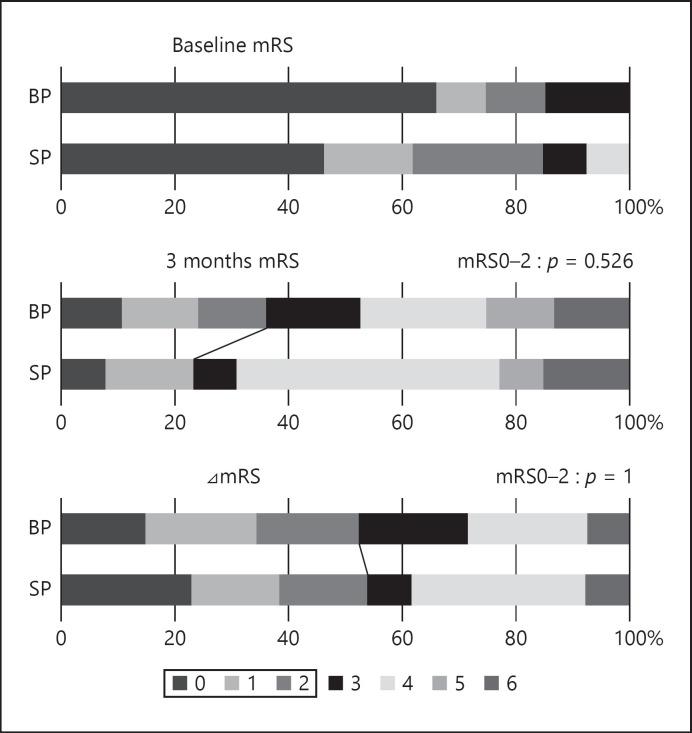
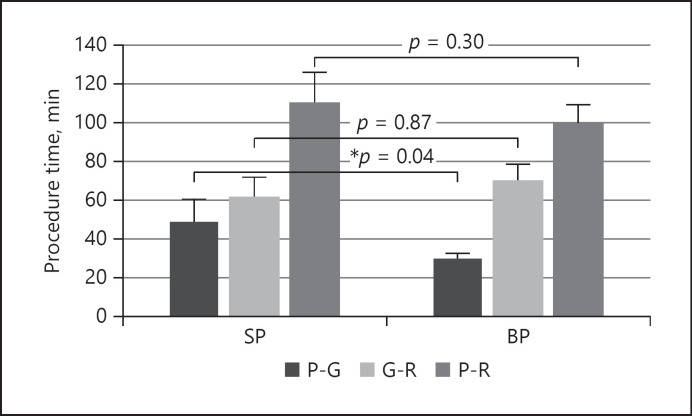
Methods: The subjects included 80 consecutive patients with anterior circulation infarction who underwent MT at our hospital between May 2015 and December 2020. Demographics and characteristics of the BP and SP groups were assessed and compared. The time from puncture to guiding catheter placement (P-G), time from guiding catheter placement to recanalization (G-R), and time from puncture to recanalization (P-R) were also extracted. A good outcome was defined as a modified Rankin scale score ≤2 at 3 months.
Results: Of the 80 patients, 67 and 13 were treated with BP and SP angiosuites, respectively. There were no differences in age, sex, complications, Alberta Stroke Program Early CT Score, National Institutes of Health Stroke Scale score at onset, occlusion site, rate of recombinant tissue-type plasminogen activator administration, stroke subtype, recanalization rate, and complications between the 2 groups. The rate of a good outcome was not different between the 2 groups. P-G was significantly longer in the SP group than in the BP group, whereas there was no significant difference in G-R and P-R between the 2 groups (P-G: BP 29.9 ± 21.8 vs. SP 48.5 ± 43.6 min, p = 0.04).
Conclusion: MT performed on the SP angiosuite tended to prolong the time for guiding catheter placement. However, there was no difference in the overall procedure time, recanalization rate, or outcome between BP and SP angiosuites. Therefore, if the BP angiosuite is not available, the use of the SP angiosuite should be encouraged.
导言:机械取栓(MT)通常在双平面(BP)血管套件上进行。当不能使用BP血管套件时,单平面(SP)血管套件可以作为替代。然而,在SP血管套件上进行MT的可行性还有待阐明。因此,我们研究了SP血管套件对前循环梗死患者手术时间、再通率和预后的详细划分的替代作用。方法:选取2015年5月至2020年12月在我院连续行MT治疗的前循环梗死患者80例。评估和比较BP组和SP组的人口统计学和特征。提取穿刺至置管时间(P-G)、置管至再通时间(G-R)、穿刺至再通时间(P-R)。3个月时改良Rankin量表评分≤2分为良好预后。结果:80例患者中,分别有67例和13例接受了BP和SP血管套件治疗。两组患者在年龄、性别、并发症、Alberta卒中Program早期CT评分、发病时美国国立卫生研究院卒中量表评分、闭塞部位、重组组织型纤溶酶原激活剂给药率、卒中亚型、再通率、并发症等方面均无差异。两组间良好预后率无差异。SP组p - g明显长于BP组,而两组间G-R、p - r差异无统计学意义(p - g: BP 29.9±21.8 min vs. SP 48.5±43.6 min, p = 0.04)。结论:在SP血管套上行MT有延长导管放置时间的趋势。然而,在总体手术时间、再通率或结果上,BP和SP血管插管没有差异。因此,如果不能使用BP血管套件,则应鼓励使用SP血管套件。
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
