{"title":"A Rare Case of Fatal Hemorrhagic Stroke in a Young Female with Early Mixed Connective Tissue Disease.","authors":"James R Agapoff Iv","doi":"10.1155/2021/5321438","DOIUrl":null,"url":null,"abstract":"<p><p>Mixed connective tissue disease (MCTD) often presents as a slow progressive illness with low morbidity and mortality. Serious central nervous system disease is uncommon, and fatal outcomes are rarely seen. Here, we report a rare case of fatal hemorrhagic stroke in a 43-year-old female with a rapidly progressive MCTD. She presented to primary care with a history of headaches, visual disturbances, and unprovoked lower extremity swelling and pain. A rheumatological workup showed positive antinuclear (ANA) and ribonucleoprotein (RNP) antibodies. Magnetic resonance imaging (MRI) found a 12 mm hemorrhage along a cortical sulcus of the right frontal lobe, and a follow-up magnetic resonance angiography (MRA) and ophthalmological exam showed no definitive signs of vasculitis. Over the course of her workup, she developed swollen hands, Raynaud's syndrome, myalgias, and synovitis characteristic of evolving MCTD. The patient then began to experience severe headaches over one month. Repeat MRI was ordered, but never completed, and the patient presented to the emergency department (ED) with a severe, right-sided headache, and left-sided visual disturbance. In the ED, she began to display evidence of delirium and seizure activity and became unresponsive. A computerized tomography scan (CT) of the brain showed a right parietal lobe intraparenchymal hemorrhage approximately 5 × 3 × 5 cm in size with secondary mass effect including mid- and hind-brain herniation. Computerized tomography angiography (CTA) of the brain showed signs of large vessel vasculitis. A craniectomy was performed; however, the patient never regained consciousness and died several days later. Vasculitis, while rare in connective tissue diseases, should be aggressively assessed for and managed in patients with any early signs and symptoms of cerebrovascular involvement to prevent fatal outcomes.</p>","PeriodicalId":9622,"journal":{"name":"Case Reports in Rheumatology","volume":"2021 ","pages":"5321438"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8568535/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5321438","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
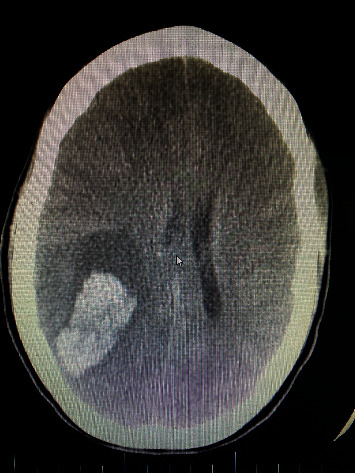
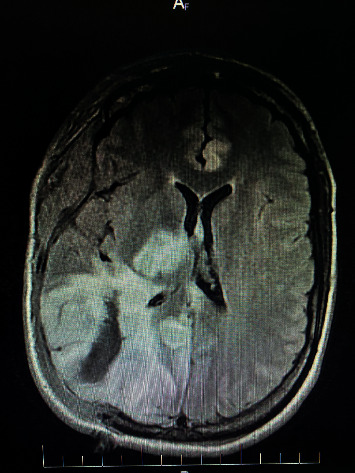
Mixed connective tissue disease (MCTD) often presents as a slow progressive illness with low morbidity and mortality. Serious central nervous system disease is uncommon, and fatal outcomes are rarely seen. Here, we report a rare case of fatal hemorrhagic stroke in a 43-year-old female with a rapidly progressive MCTD. She presented to primary care with a history of headaches, visual disturbances, and unprovoked lower extremity swelling and pain. A rheumatological workup showed positive antinuclear (ANA) and ribonucleoprotein (RNP) antibodies. Magnetic resonance imaging (MRI) found a 12 mm hemorrhage along a cortical sulcus of the right frontal lobe, and a follow-up magnetic resonance angiography (MRA) and ophthalmological exam showed no definitive signs of vasculitis. Over the course of her workup, she developed swollen hands, Raynaud's syndrome, myalgias, and synovitis characteristic of evolving MCTD. The patient then began to experience severe headaches over one month. Repeat MRI was ordered, but never completed, and the patient presented to the emergency department (ED) with a severe, right-sided headache, and left-sided visual disturbance. In the ED, she began to display evidence of delirium and seizure activity and became unresponsive. A computerized tomography scan (CT) of the brain showed a right parietal lobe intraparenchymal hemorrhage approximately 5 × 3 × 5 cm in size with secondary mass effect including mid- and hind-brain herniation. Computerized tomography angiography (CTA) of the brain showed signs of large vessel vasculitis. A craniectomy was performed; however, the patient never regained consciousness and died several days later. Vasculitis, while rare in connective tissue diseases, should be aggressively assessed for and managed in patients with any early signs and symptoms of cerebrovascular involvement to prevent fatal outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
