Twenty years of integrated disease surveillance and response in Sub-Saharan Africa: challenges and opportunities for effective management of infectious disease epidemics.
Irene R Mremi, Janeth George, Susan F Rumisha, Calvin Sindato, Sharadhuli I Kimera, Leonard E G Mboera
{"title":"Twenty years of integrated disease surveillance and response in Sub-Saharan Africa: challenges and opportunities for effective management of infectious disease epidemics.","authors":"Irene R Mremi, Janeth George, Susan F Rumisha, Calvin Sindato, Sharadhuli I Kimera, Leonard E G Mboera","doi":"10.1186/s42522-021-00052-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>This systematic review aimed to analyse the performance of the Integrated Disease Surveillance and Response (IDSR) strategy in Sub-Saharan Africa (SSA) and how its implementation has embraced advancement in information technology, big data analytics techniques and wealth of data sources.</p><p><strong>Methods: </strong>HINARI, PubMed, and advanced Google Scholar databases were searched for eligible articles. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols.</p><p><strong>Results: </strong>A total of 1,809 articles were identified and screened at two stages. Forty-five studies met the inclusion criteria, of which 35 were country-specific, seven covered the SSA region, and three covered 3-4 countries. Twenty-six studies assessed the IDSR core functions, 43 the support functions, while 24 addressed both functions. Most of the studies involved Tanzania (9), Ghana (6) and Uganda (5). The routine Health Management Information System (HMIS), which collects data from health care facilities, has remained the primary source of IDSR data. However, the system is characterised by inadequate data completeness, timeliness, quality, analysis and utilisation, and lack of integration of data from other sources. Under-use of advanced and big data analytical technologies in performing disease surveillance and relating multiple indicators minimises the optimisation of clinical and practice evidence-based decision-making.</p><p><strong>Conclusions: </strong>This review indicates that most countries in SSA rely mainly on traditional indicator-based disease surveillance utilising data from healthcare facilities with limited use of data from other sources. It is high time that SSA countries consider and adopt multi-sectoral, multi-disease and multi-indicator platforms that integrate other sources of health information to provide support to effective detection and prompt response to public health threats.</p>","PeriodicalId":19490,"journal":{"name":"One Health Outlook","volume":"3 1","pages":"22"},"PeriodicalIF":0.0000,"publicationDate":"2021-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8575546/pdf/","citationCount":"19","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"One Health Outlook","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42522-021-00052-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 19
Abstract
Introduction: This systematic review aimed to analyse the performance of the Integrated Disease Surveillance and Response (IDSR) strategy in Sub-Saharan Africa (SSA) and how its implementation has embraced advancement in information technology, big data analytics techniques and wealth of data sources.
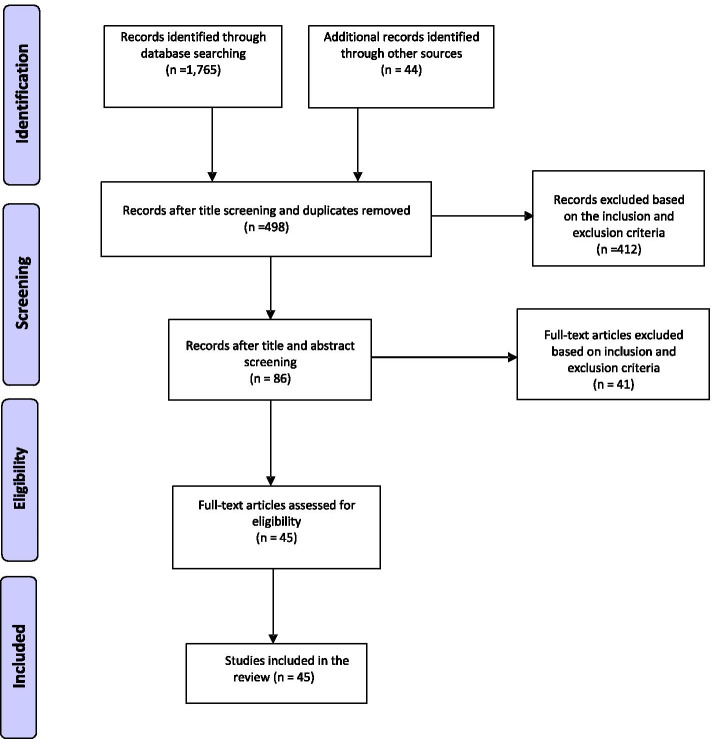
Methods: HINARI, PubMed, and advanced Google Scholar databases were searched for eligible articles. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols.
Results: A total of 1,809 articles were identified and screened at two stages. Forty-five studies met the inclusion criteria, of which 35 were country-specific, seven covered the SSA region, and three covered 3-4 countries. Twenty-six studies assessed the IDSR core functions, 43 the support functions, while 24 addressed both functions. Most of the studies involved Tanzania (9), Ghana (6) and Uganda (5). The routine Health Management Information System (HMIS), which collects data from health care facilities, has remained the primary source of IDSR data. However, the system is characterised by inadequate data completeness, timeliness, quality, analysis and utilisation, and lack of integration of data from other sources. Under-use of advanced and big data analytical technologies in performing disease surveillance and relating multiple indicators minimises the optimisation of clinical and practice evidence-based decision-making.
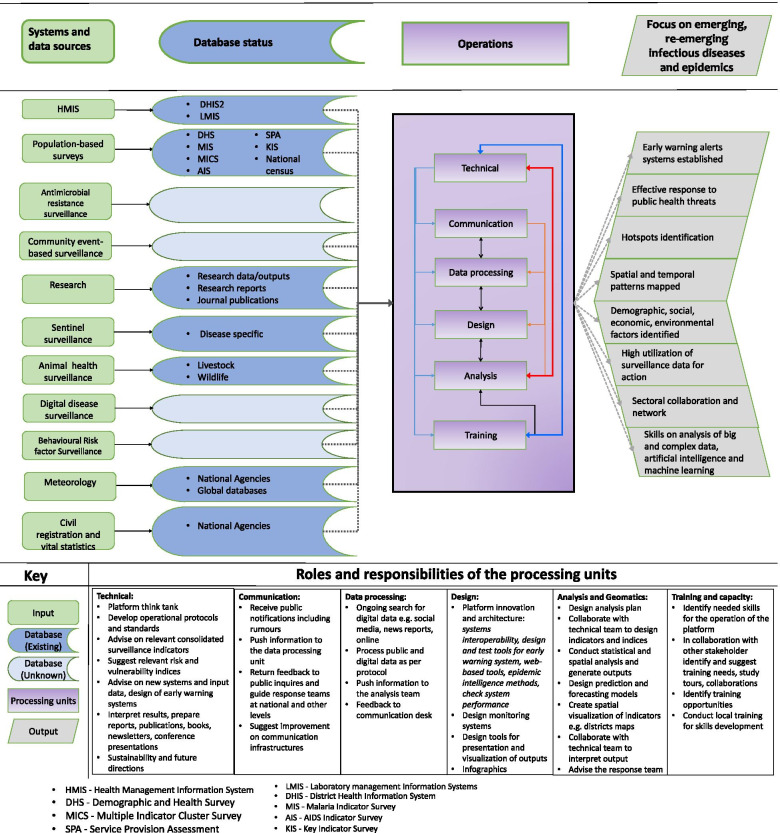
Conclusions: This review indicates that most countries in SSA rely mainly on traditional indicator-based disease surveillance utilising data from healthcare facilities with limited use of data from other sources. It is high time that SSA countries consider and adopt multi-sectoral, multi-disease and multi-indicator platforms that integrate other sources of health information to provide support to effective detection and prompt response to public health threats.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
