{"title":"Y Stent Rendezvous to Treat Symptomatic Innominate Artery Stenosis.","authors":"Goran Mitreski, Hamed Asadi, Mark Duncan Brooks","doi":"10.5469/neuroint.2021.00472","DOIUrl":null,"url":null,"abstract":"<p><p>A male in his 60s presented with transient ischemic attacks 5 years after aortic arch branch graft repair for type A aortic dissection. Computed tomographic angiography demonstrated 80% stenosis of the brachiocephalic artery close to the origins of the right common carotid and subclavian arteries. The case was reviewed at our multidisciplinary aortic meeting and a plan for endovascular management was made. Percutaneous endovascular Y stenting from the innominate artery into the left common carotid and subclavian arteries was achieved using self-expanding nitinol stents with a rendezvous technique that included retrograde right radial artery, retrograde right external carotid artery, and retrograde right femoral arterial approaches. At 6 months review, the stents remained widely patent and the patient was symptom-free.</p>","PeriodicalId":19140,"journal":{"name":"Neurointervention","volume":"17 1","pages":"45-49"},"PeriodicalIF":1.2000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c1/20/neuroint-2021-00472.PMC8891582.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurointervention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5469/neuroint.2021.00472","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/14 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
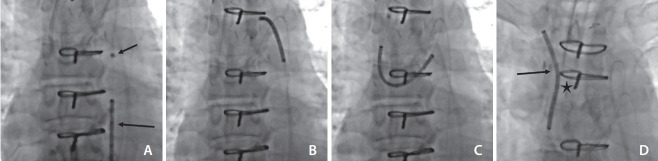
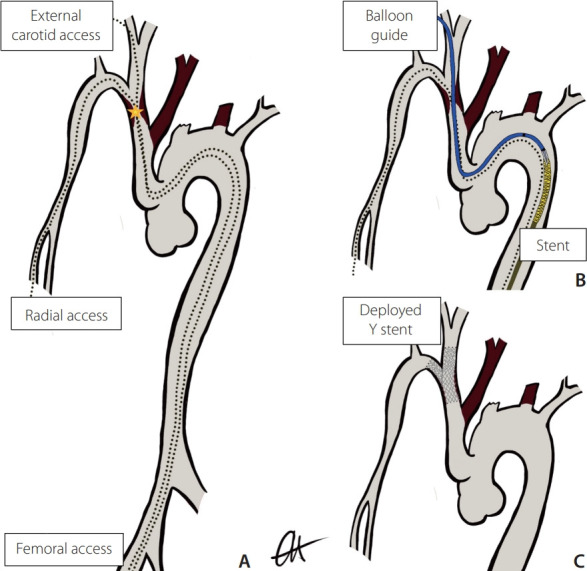
A male in his 60s presented with transient ischemic attacks 5 years after aortic arch branch graft repair for type A aortic dissection. Computed tomographic angiography demonstrated 80% stenosis of the brachiocephalic artery close to the origins of the right common carotid and subclavian arteries. The case was reviewed at our multidisciplinary aortic meeting and a plan for endovascular management was made. Percutaneous endovascular Y stenting from the innominate artery into the left common carotid and subclavian arteries was achieved using self-expanding nitinol stents with a rendezvous technique that included retrograde right radial artery, retrograde right external carotid artery, and retrograde right femoral arterial approaches. At 6 months review, the stents remained widely patent and the patient was symptom-free.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
