Sarah Alexandra van Blydenstein, Colin Nigel Menezes, Nicole Miller, Naomi Johnson, Bavinash Pillay, Barry F Jacobson, Shahed Omar
{"title":"Prevalence and Trajectory of COVID-19-Associated Hypercoagulability Using Serial Thromboelastography in a South African Population.","authors":"Sarah Alexandra van Blydenstein, Colin Nigel Menezes, Nicole Miller, Naomi Johnson, Bavinash Pillay, Barry F Jacobson, Shahed Omar","doi":"10.1155/2021/3935098","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The coagulation abnormalities resulting from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been attributed to inflammation and subsequent cytokine storm. Thromboelastography (TEG) is a point-of-care test used to assess clot formation and degradation in whole blood and is an indicator of the overall real-time coagulopathic state of the patient.</p><p><strong>Methods: </strong>A single-centre, prospective, observational cohort study was conducted in South Africa, analysing the coagulation patterns of 41 patients with hypoxia related to SARS-CoV-2 using serial thromboelastography (TEG) on admission, after 48 hours, and at resolution of hypoxia/day 10. Results: Two-thirds (<i>n</i> = 26) were women. The median age was 61 (IQR 50-67), and the majority (88%) were Black patients. Almost half (22) of the patients were critically ill and ventilated, with median SOFA and SAPS2 scores of 3 and 22 (IQR2-4 and 18-30), respectively. The prevalence of hypercoagulability was 0.54 (95% CI 0.46-0.62), whilst 29/41 (0.71, CI 0.64-0.78)) met the definition of hypofibrinolysis. Differences between the hypercoagulable (HC) and non-hypercoagulable groups remained apparent at 48 hours after anticoagulation. At this time point, the K time was significantly lower (<i>p</i> ˂ 0,01), and the <i>α</i>-angle (<i>p</i> ˂ 0,01) and maximum amplitude (MA) (<i>p</i> ˂ 0,01) were significantly higher in the HC cohort. At resolution of hypoxia, or day 10, only MA was significantly higher in the hypercoagulable group compared to the non-hypercoagulable group (<i>p</i> = 0.01). The initial impairment in fibrinolysis (Ly30), <i>α</i> angle, and MA were significantly associated with mortality, with <i>p</i> values of 0.006, 0.031, and 0.04, respectively.</p><p><strong>Conclusions: </strong>In this South African population, hypercoagulability was a highly prevalent phenomenon in COVID-19 disease. It was typified by hypofibrinolysis and a persistently elevated MA, despite anticoagulation therapy.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":" ","pages":"3935098"},"PeriodicalIF":1.8000,"publicationDate":"2021-12-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8694947/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/3935098","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: The coagulation abnormalities resulting from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been attributed to inflammation and subsequent cytokine storm. Thromboelastography (TEG) is a point-of-care test used to assess clot formation and degradation in whole blood and is an indicator of the overall real-time coagulopathic state of the patient.
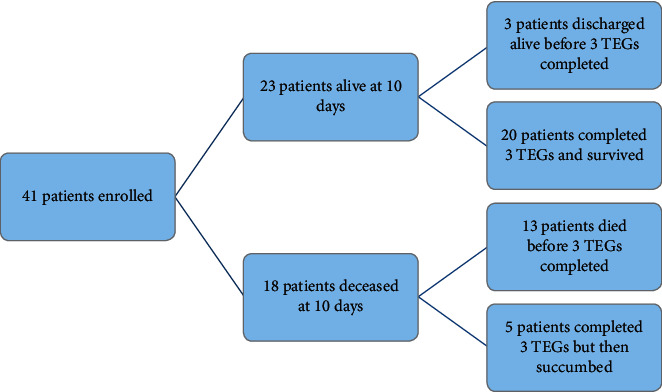
Methods: A single-centre, prospective, observational cohort study was conducted in South Africa, analysing the coagulation patterns of 41 patients with hypoxia related to SARS-CoV-2 using serial thromboelastography (TEG) on admission, after 48 hours, and at resolution of hypoxia/day 10. Results: Two-thirds (n = 26) were women. The median age was 61 (IQR 50-67), and the majority (88%) were Black patients. Almost half (22) of the patients were critically ill and ventilated, with median SOFA and SAPS2 scores of 3 and 22 (IQR2-4 and 18-30), respectively. The prevalence of hypercoagulability was 0.54 (95% CI 0.46-0.62), whilst 29/41 (0.71, CI 0.64-0.78)) met the definition of hypofibrinolysis. Differences between the hypercoagulable (HC) and non-hypercoagulable groups remained apparent at 48 hours after anticoagulation. At this time point, the K time was significantly lower (p ˂ 0,01), and the α-angle (p ˂ 0,01) and maximum amplitude (MA) (p ˂ 0,01) were significantly higher in the HC cohort. At resolution of hypoxia, or day 10, only MA was significantly higher in the hypercoagulable group compared to the non-hypercoagulable group (p = 0.01). The initial impairment in fibrinolysis (Ly30), α angle, and MA were significantly associated with mortality, with p values of 0.006, 0.031, and 0.04, respectively.
Conclusions: In this South African population, hypercoagulability was a highly prevalent phenomenon in COVID-19 disease. It was typified by hypofibrinolysis and a persistently elevated MA, despite anticoagulation therapy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
