Transesophageal echocardiography and risk of respiratory failure in patients who had ischemic stroke or transient ischemic attack: an IDEAL phase 4 study.
Samuel S Bruce, Babak B Navi, Cenai Zhang, Jiwon Kim, Richard B Devereux, Edward J Schenck, Art Sedrakyan, Iván Díaz, Hooman Kamel
{"title":"Transesophageal echocardiography and risk of respiratory failure in patients who had ischemic stroke or transient ischemic attack: an IDEAL phase 4 study.","authors":"Samuel S Bruce, Babak B Navi, Cenai Zhang, Jiwon Kim, Richard B Devereux, Edward J Schenck, Art Sedrakyan, Iván Díaz, Hooman Kamel","doi":"10.1136/bmjsit-2021-000116","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Transesophageal echocardiography (TEE) is sometimes used to search for cardioembolic sources after ischemic stroke or transient ischemic attack (TIA). TEE visualizes some sources better than transthoracic echocardiography, but TEE is invasive and may cause aspiration. Few data exist on the risk of respiratory complications after TEE in patients who had stroke or TIA. Our objective was to determine whether TEE was associated with increased risk of respiratory failure in patients who had ischemic stroke or TIA.</p><p><strong>Design: </strong>This is a retrospective cohort study using administrative data from inpatient and outpatient insurance claims collected by the US federal government's Centers for Medicare and Medicaid Services.</p><p><strong>Setting: </strong>Hospitals and outpatient clinics throughout the USA.</p><p><strong>Participants: </strong>99 081 patients ≥65 years old hospitalized for out-of-hospital ischemic stroke or TIA, defined by validated International Classification of Disease-9/10 diagnosis codes and present-on-admission codes, using claims data from 2008 to 2018 in a random 5% sample of Medicare beneficiaries.</p><p><strong>Main outcome measures: </strong>Acute respiratory failure, defined as endotracheal intubation and/or mechanical ventilation, starting on the first day after admission through 28 days afterward.</p><p><strong>Results: </strong>Of 99 081 patients included in this analysis, 73 733 (74.4%) had an ischemic stroke and 25 348 (25.6%) a TIA. TEE was performed in 4677 (4.7%) patients and intubation and/or mechanical ventilation in 1403 (1.4%) patients. The 28-day cumulative risk of respiratory failure after TEE (1.4%; 95% CI 0.8% to 2.7%) was similar to that seen in those without TEE (1.4%; 95% CI 1.4% to 1.5%) (p=0.84). After adjustment for age, sex, race, Charlson comorbidities, diagnosis of stroke versus TIA, intravenous thrombolysis, and mechanical thrombectomy, TEE was not associated with an increased risk of respiratory failure (HR, 0.9; 95% CI 0.6 to 1.2).</p><p><strong>Conclusions: </strong>In a cohort of older patients who had ischemic stroke or TIA, TEE was not associated with an increased risk of subsequent respiratory failure.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":" ","pages":"e000116"},"PeriodicalIF":1.6000,"publicationDate":"2022-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/94/18/bmjsit-2021-000116.PMC8823208.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2021-000116","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 3
Abstract
Objective: Transesophageal echocardiography (TEE) is sometimes used to search for cardioembolic sources after ischemic stroke or transient ischemic attack (TIA). TEE visualizes some sources better than transthoracic echocardiography, but TEE is invasive and may cause aspiration. Few data exist on the risk of respiratory complications after TEE in patients who had stroke or TIA. Our objective was to determine whether TEE was associated with increased risk of respiratory failure in patients who had ischemic stroke or TIA.
Design: This is a retrospective cohort study using administrative data from inpatient and outpatient insurance claims collected by the US federal government's Centers for Medicare and Medicaid Services.
Setting: Hospitals and outpatient clinics throughout the USA.
Participants: 99 081 patients ≥65 years old hospitalized for out-of-hospital ischemic stroke or TIA, defined by validated International Classification of Disease-9/10 diagnosis codes and present-on-admission codes, using claims data from 2008 to 2018 in a random 5% sample of Medicare beneficiaries.
Main outcome measures: Acute respiratory failure, defined as endotracheal intubation and/or mechanical ventilation, starting on the first day after admission through 28 days afterward.
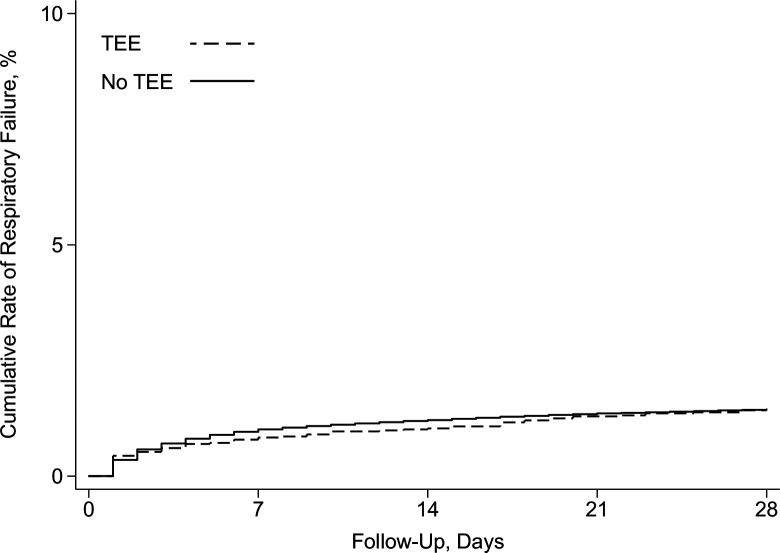
Results: Of 99 081 patients included in this analysis, 73 733 (74.4%) had an ischemic stroke and 25 348 (25.6%) a TIA. TEE was performed in 4677 (4.7%) patients and intubation and/or mechanical ventilation in 1403 (1.4%) patients. The 28-day cumulative risk of respiratory failure after TEE (1.4%; 95% CI 0.8% to 2.7%) was similar to that seen in those without TEE (1.4%; 95% CI 1.4% to 1.5%) (p=0.84). After adjustment for age, sex, race, Charlson comorbidities, diagnosis of stroke versus TIA, intravenous thrombolysis, and mechanical thrombectomy, TEE was not associated with an increased risk of respiratory failure (HR, 0.9; 95% CI 0.6 to 1.2).
Conclusions: In a cohort of older patients who had ischemic stroke or TIA, TEE was not associated with an increased risk of subsequent respiratory failure.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
