Shuktika Nandkeolyar, Tanya Doctorian, Gary Fraser, Rachel Ryu, Colleen Fearon, David Tryon, Whitney Kagabo, Dmitry Abramov, Christopher Hauschild, Liset Stoletniy, Anthony Hilliard, Antoine Sakr
{"title":"Predictors of In-hospital Mortality in Cardiogenic Shock Patients on Vasoactive or Inotropic Support.","authors":"Shuktika Nandkeolyar, Tanya Doctorian, Gary Fraser, Rachel Ryu, Colleen Fearon, David Tryon, Whitney Kagabo, Dmitry Abramov, Christopher Hauschild, Liset Stoletniy, Anthony Hilliard, Antoine Sakr","doi":"10.1177/11795468211049449","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Though controversial, the short-duration in-patient use of inotropes in cardiogenic shock (CS) remain an ACC/AHA Class IIa indication, and are frequently used in the initial treatment of CS. We evaluated in-patient mortality and effect on mortality risk of commonly used vasoactive inotropic medications for the medical management of SCAI stage B and C cardiogenic shock patients in a tertiary care cardiac care unit: dobutamine, dopamine, milrinone, and norepinephrine.</p><p><strong>Methods: </strong>We retrospectively evaluated 342 patients who received dobutamine, milrinone, dopamine, norepinephrine or a combination of these medications for SCAI stage B and C cardiogenic shock. Cox proportional hazards were used to form longitudinal mortality predictions.</p><p><strong>Results: </strong>Overall in-patient mortality was 18%. Each 1 µg/kg/minute increase in dobutamine independently corresponded to a 15% increase in risk of mortality. High dose dobutamine >3 µg/kg/minute is associated with 3-fold increased risk compared to ⩽3 µg/kg/minute (<i>P</i> < .001). Use of milrinone, norepinephrine, and dopamine were not independently associated with mortality.</p><p><strong>Conclusion: </strong>We demonstrate that the overall in-hospital mortality of SCAI stage B and C cardiogenic shock patients medically managed on inotropes was not in excess of prior studies. Dobutamine was independently associated with mortality, while other vasoactive inotropic medications were not. Inotropes remain a feasible method of managing SCAI stage B and C cardiogenic shock.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"15 ","pages":"11795468211049449"},"PeriodicalIF":3.3000,"publicationDate":"2021-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7c/35/10.1177_11795468211049449.PMC8554565.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468211049449","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Though controversial, the short-duration in-patient use of inotropes in cardiogenic shock (CS) remain an ACC/AHA Class IIa indication, and are frequently used in the initial treatment of CS. We evaluated in-patient mortality and effect on mortality risk of commonly used vasoactive inotropic medications for the medical management of SCAI stage B and C cardiogenic shock patients in a tertiary care cardiac care unit: dobutamine, dopamine, milrinone, and norepinephrine.
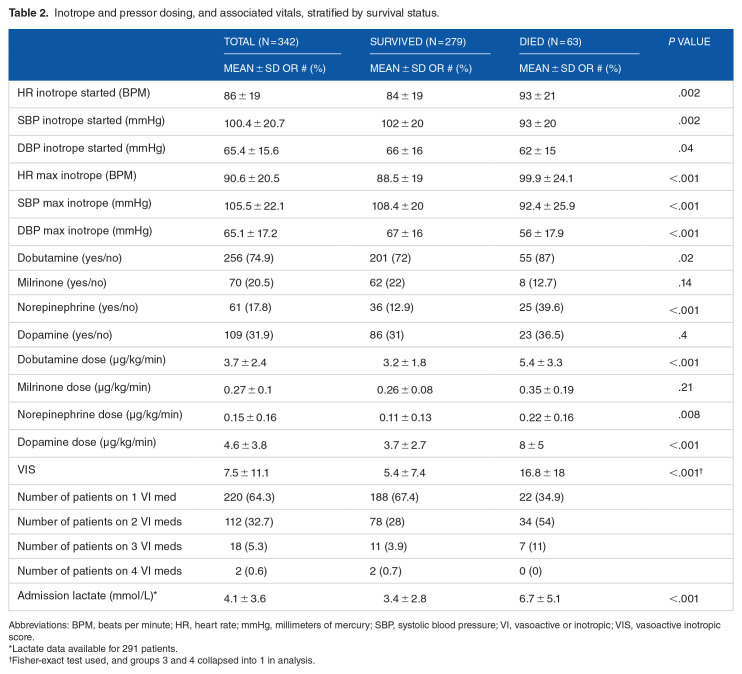
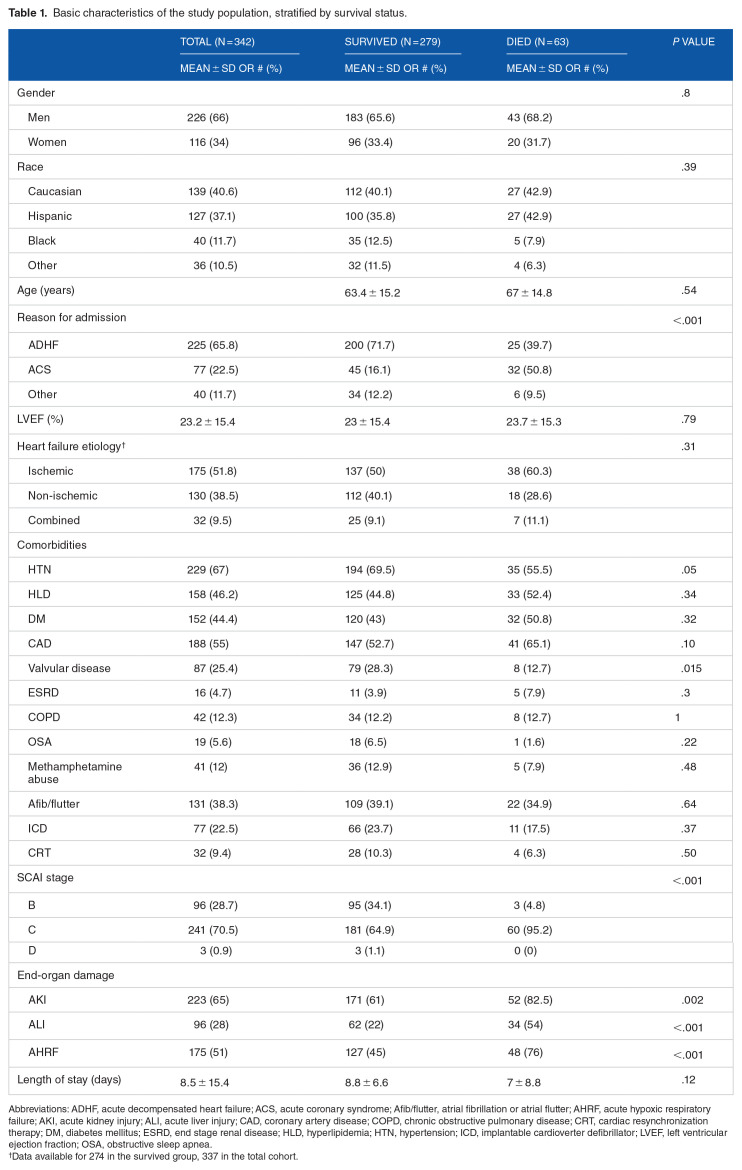
Methods: We retrospectively evaluated 342 patients who received dobutamine, milrinone, dopamine, norepinephrine or a combination of these medications for SCAI stage B and C cardiogenic shock. Cox proportional hazards were used to form longitudinal mortality predictions.
Results: Overall in-patient mortality was 18%. Each 1 µg/kg/minute increase in dobutamine independently corresponded to a 15% increase in risk of mortality. High dose dobutamine >3 µg/kg/minute is associated with 3-fold increased risk compared to ⩽3 µg/kg/minute (P < .001). Use of milrinone, norepinephrine, and dopamine were not independently associated with mortality.
Conclusion: We demonstrate that the overall in-hospital mortality of SCAI stage B and C cardiogenic shock patients medically managed on inotropes was not in excess of prior studies. Dobutamine was independently associated with mortality, while other vasoactive inotropic medications were not. Inotropes remain a feasible method of managing SCAI stage B and C cardiogenic shock.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
