Luca F Valle, Nicholas Bernthal, Fritz C Eilber, Jacob E Shabason, Meena Bedi, Anusha Kalbasi
{"title":"Evaluating Thresholds to Adopt Hypofractionated Preoperative Radiotherapy as Standard of Care in Sarcoma.","authors":"Luca F Valle, Nicholas Bernthal, Fritz C Eilber, Jacob E Shabason, Meena Bedi, Anusha Kalbasi","doi":"10.1155/2021/3735874","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Data supporting hypofractionated preoperative radiation therapy (RT) for patients with extremity and trunk soft tissue sarcoma (STS) are currently limited to phase II single-institution studies. We sought to understand the type and thresholds of clinical evidence required for experts to adopt hypofractionated RT as a standard-of-care option for patients with STS.</p><p><strong>Methods: </strong>An electronic survey was distributed to multidisciplinary sarcoma experts. The survey queried whether data from a theoretical, multi-institutional, phase II study of 5-fraction preoperative RT could change practice. Using endpoints from RTOG 0630 as a reference, the survey also queried thresholds for acceptable local control, wound complication, and late toxicity for the study protocol to be accepted as a standard-of-care option. Responses were logged from 8/27/2020 to 9/8/2020 and summarized graphically.</p><p><strong>Results: </strong>The survey response rate was 55.3% (47/85). Local control is the most important clinical outcome for sarcoma specialists when evaluating whether an RT regimen should be considered standard of care. 17% (8/47) of providers require randomized phase III evidence to consider hypofractionated preoperative RT as a standard-of-care option, whereas 10.6% (5/47) of providers already view this as a standard-of-care option. Of providers willing to change practice based on phase II data, most (78%, 29/37) would accept local control rates equivalent to or less than those in RTOG 0630, as long as the rate was higher than 85%. However, 51.3% (19/37) would require wound complication rates superior to those reported in RTOG 0630, and 46% (17/37) of respondents would accept late toxicity rates inferior to RTOG 0630.</p><p><strong>Conclusion: </strong>Consensus building is needed among clinicians regarding the type and threshold of evidence needed to evaluate hypofractionated RT as a standard-of-care option. A collaborative consortium-based approach may be the most pragmatic means for developing consensus protocols and pooling data to gradually introduce hypofractionated preoperative RT into routine practice.</p>","PeriodicalId":21431,"journal":{"name":"Sarcoma","volume":"2021 ","pages":"3735874"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8556117/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sarcoma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/3735874","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Data supporting hypofractionated preoperative radiation therapy (RT) for patients with extremity and trunk soft tissue sarcoma (STS) are currently limited to phase II single-institution studies. We sought to understand the type and thresholds of clinical evidence required for experts to adopt hypofractionated RT as a standard-of-care option for patients with STS.
Methods: An electronic survey was distributed to multidisciplinary sarcoma experts. The survey queried whether data from a theoretical, multi-institutional, phase II study of 5-fraction preoperative RT could change practice. Using endpoints from RTOG 0630 as a reference, the survey also queried thresholds for acceptable local control, wound complication, and late toxicity for the study protocol to be accepted as a standard-of-care option. Responses were logged from 8/27/2020 to 9/8/2020 and summarized graphically.
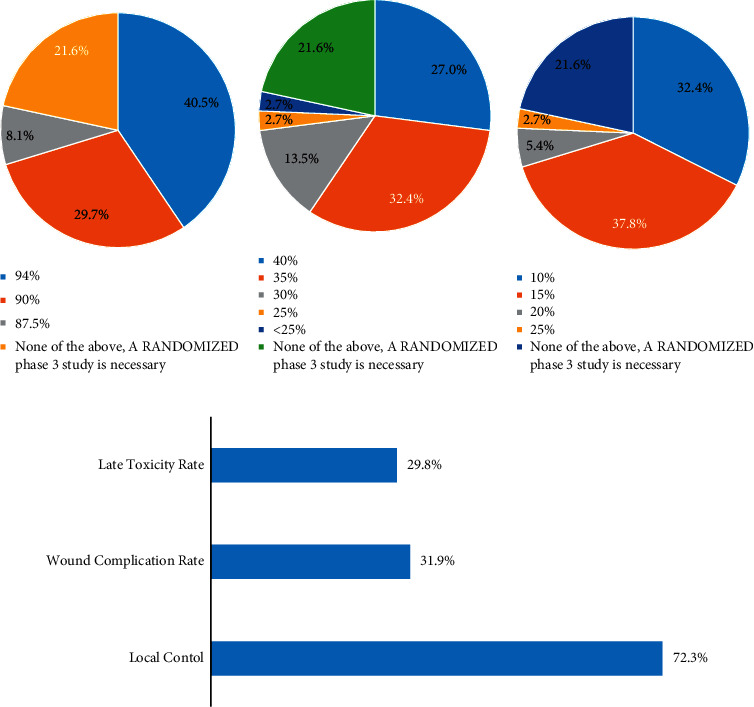
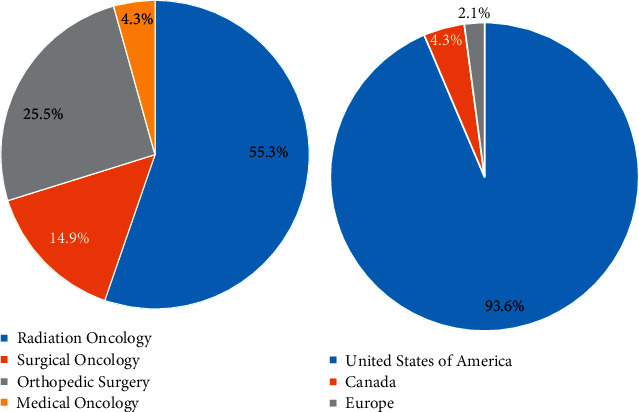
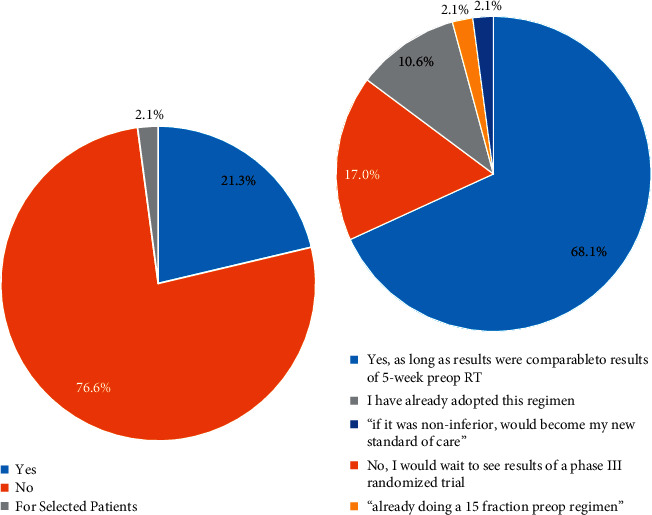
Results: The survey response rate was 55.3% (47/85). Local control is the most important clinical outcome for sarcoma specialists when evaluating whether an RT regimen should be considered standard of care. 17% (8/47) of providers require randomized phase III evidence to consider hypofractionated preoperative RT as a standard-of-care option, whereas 10.6% (5/47) of providers already view this as a standard-of-care option. Of providers willing to change practice based on phase II data, most (78%, 29/37) would accept local control rates equivalent to or less than those in RTOG 0630, as long as the rate was higher than 85%. However, 51.3% (19/37) would require wound complication rates superior to those reported in RTOG 0630, and 46% (17/37) of respondents would accept late toxicity rates inferior to RTOG 0630.
Conclusion: Consensus building is needed among clinicians regarding the type and threshold of evidence needed to evaluate hypofractionated RT as a standard-of-care option. A collaborative consortium-based approach may be the most pragmatic means for developing consensus protocols and pooling data to gradually introduce hypofractionated preoperative RT into routine practice.
SarcomaMedicine-Radiology, Nuclear Medicine and Imaging
CiteScore
5.00
自引率
0.00%
发文量
15
审稿时长
14 weeks
期刊介绍:
Sarcoma is dedicated to publishing papers covering all aspects of connective tissue oncology research. It brings together work from scientists and clinicians carrying out a broad range of research in this field, including the basic sciences, molecular biology and pathology and the clinical sciences of epidemiology, surgery, radiotherapy and chemotherapy. High-quality papers concerning the entire range of bone and soft tissue sarcomas in both adults and children, including Kaposi"s sarcoma, are published as well as preclinical and animal studies. This journal provides a central forum for the description of advances in diagnosis, assessment and treatment of this rarely seen, but often mismanaged, group of patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
