{"title":"Scapular Winging following Sports-Related Injury in a Rugby Player.","authors":"Shinya Ishizuka, Akinori Kobayakawa, Hideki Hiraiwa, Hiroki Oba, Takefumi Sakaguchi, Masaru Idota, Takahiro Haga, Takafumi Mizuno, Itaru Kawashima, Kanae Kuriyama, Shiro Imagama","doi":"10.1155/2021/4511538","DOIUrl":null,"url":null,"abstract":"<p><p>The most common cause of medial scapular winging is long thoracic nerve palsy (LTN) and subsequent serratus anterior muscle dysfunction. A 16-year-old right-handed male high-school rugby player developed severe right-sided neck and shoulder pain after tackling an opponent while playing rugby. Six weeks after initial injury, the patient observed shoulder muscle weakness when performing his daily activities. On physical examination, limited active elevation of the right shoulder in the scapular plane and scapular winging was observed. Magnetic resonance imaging revealed atrophy of both the SA and subclavius muscles on the right side, and we initially suspected an LTN injury sustained. However, while detailing his history, the patient explained that he also had noted difficulty sucking high viscosity drinks such as shakes and smoothies since childhood. In addition, physical examination showed weakness of the orbicularis oculi muscle. Considering the facial muscle weakness, facioscapulohumeral dystrophy (FSHD) was also suspected, and genetic testing showed chromosome 4q35 deletion with restriction fragments 17 kb and 3 tandem repeated DNA confirming the diagnosis of FSHD. Clinicians should be aware that FSHD could be one of the differential diagnoses of scapular winging after sports injury, and surgeons should rule out the diagnosis of FSHD before performing any surgical treatment for SA palsy.</p>","PeriodicalId":30287,"journal":{"name":"Case Reports in Orthopedics","volume":"2021 ","pages":"4511538"},"PeriodicalIF":0.6000,"publicationDate":"2021-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8564197/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/4511538","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
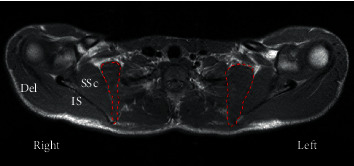
The most common cause of medial scapular winging is long thoracic nerve palsy (LTN) and subsequent serratus anterior muscle dysfunction. A 16-year-old right-handed male high-school rugby player developed severe right-sided neck and shoulder pain after tackling an opponent while playing rugby. Six weeks after initial injury, the patient observed shoulder muscle weakness when performing his daily activities. On physical examination, limited active elevation of the right shoulder in the scapular plane and scapular winging was observed. Magnetic resonance imaging revealed atrophy of both the SA and subclavius muscles on the right side, and we initially suspected an LTN injury sustained. However, while detailing his history, the patient explained that he also had noted difficulty sucking high viscosity drinks such as shakes and smoothies since childhood. In addition, physical examination showed weakness of the orbicularis oculi muscle. Considering the facial muscle weakness, facioscapulohumeral dystrophy (FSHD) was also suspected, and genetic testing showed chromosome 4q35 deletion with restriction fragments 17 kb and 3 tandem repeated DNA confirming the diagnosis of FSHD. Clinicians should be aware that FSHD could be one of the differential diagnoses of scapular winging after sports injury, and surgeons should rule out the diagnosis of FSHD before performing any surgical treatment for SA palsy.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
