Carotid Artery-Cavernous Segment Injury during an Endoscopic Endonasal Surgery: A Case Report and Literature Review of the Overlooked Option for Surgical Trapping in the Hyperacute Phase.
{"title":"Carotid Artery-Cavernous Segment Injury during an Endoscopic Endonasal Surgery: A Case Report and Literature Review of the Overlooked Option for Surgical Trapping in the Hyperacute Phase.","authors":"Gokmen Kahilogullari, Burak Bahadır, Melih Bozkurt, Seray Akcalar, Sinan Balci, Anil Arat","doi":"10.1055/s-0041-1740511","DOIUrl":null,"url":null,"abstract":"<p><p>Internal carotid artery (ICA) injury is a catastrophic complication of endoscopic endonasal surgery (EES). However, its standard management, emergent endovascular treatment, may not always be available, and the transnasal approach may be insufficient to achieve hemostasis. A 44-year-old woman with pituitary adenoma underwent EES complicated with the ICA cavernous segment injury (CSI). In urgent intraoperative angiogram, a good collateral flow from the contralateral carotid circulation was observed. Due to the unavailability of intraoperative embolization, emergent surgical trapping was performed by combined transcranial and cervical approach. The patient recovered but later developed a giant cavernous pseudoaneurysm. During the pseudoaneurysm embolization, ICA was directly accessed via a 1.7-F puncture hole using a bare microcatheter technique. Then, both the aneurysm and parent artery were obliterated with coils. At the 4-year follow-up, the patient was asymptomatic without a residual tumor. To our knowledge, this is the first case of ICA-CSI during EES successfully treated with ICA trapping as a lifesaving urgent surgery that achieved a complete recovery after a pseudoaneurysm embolization. Although several studies reported that EES-related ICA-CSIs with percutaneous carotid artery access, neither our surgical salvage technique nor our carotid access and tract embolization techniques were previously described.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":"82 4","pages":"e53-e62"},"PeriodicalIF":0.7000,"publicationDate":"2021-12-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/2e/10-1055-s-0041-1740511.PMC8670996.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0041-1740511","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
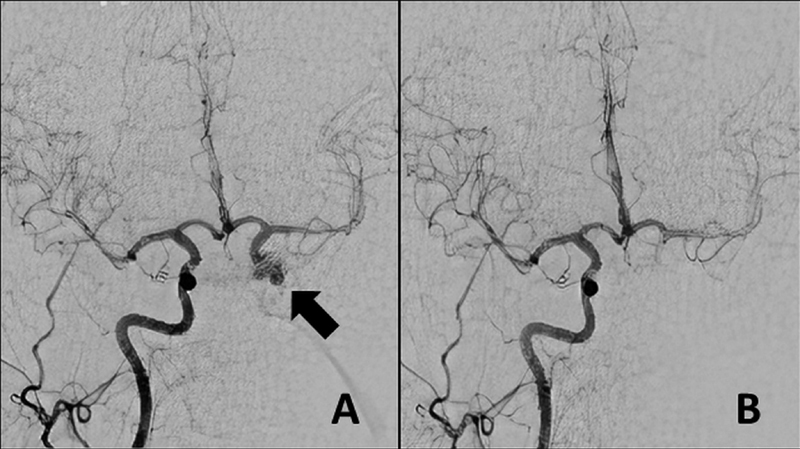
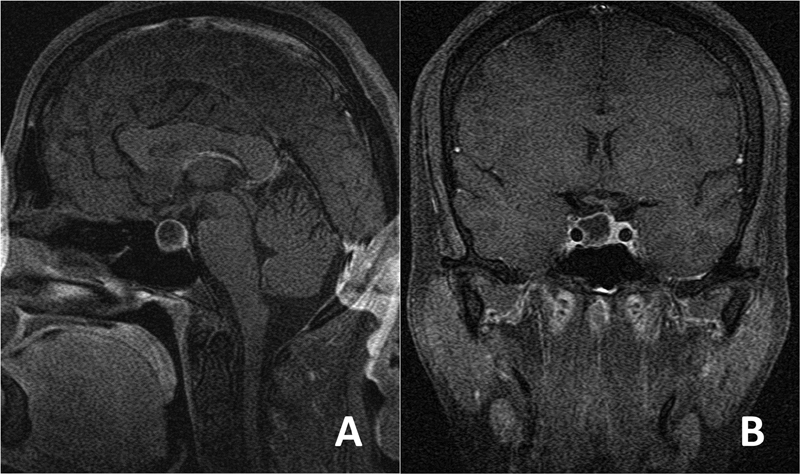
Internal carotid artery (ICA) injury is a catastrophic complication of endoscopic endonasal surgery (EES). However, its standard management, emergent endovascular treatment, may not always be available, and the transnasal approach may be insufficient to achieve hemostasis. A 44-year-old woman with pituitary adenoma underwent EES complicated with the ICA cavernous segment injury (CSI). In urgent intraoperative angiogram, a good collateral flow from the contralateral carotid circulation was observed. Due to the unavailability of intraoperative embolization, emergent surgical trapping was performed by combined transcranial and cervical approach. The patient recovered but later developed a giant cavernous pseudoaneurysm. During the pseudoaneurysm embolization, ICA was directly accessed via a 1.7-F puncture hole using a bare microcatheter technique. Then, both the aneurysm and parent artery were obliterated with coils. At the 4-year follow-up, the patient was asymptomatic without a residual tumor. To our knowledge, this is the first case of ICA-CSI during EES successfully treated with ICA trapping as a lifesaving urgent surgery that achieved a complete recovery after a pseudoaneurysm embolization. Although several studies reported that EES-related ICA-CSIs with percutaneous carotid artery access, neither our surgical salvage technique nor our carotid access and tract embolization techniques were previously described.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
