Comparison between GlideRite® rigid stylet and Parker Flex-It™ stylet to facilitate GlideScope intubation in simulated difficult intubation: a randomized controlled study.
Ji Won Bak, Yeonji Noh, Juyoun Kim, Byeongmun Hwang, Seongsik Kang, Heejeong Son, Minsoo Kim
{"title":"Comparison between GlideRite® rigid stylet and Parker Flex-It™ stylet to facilitate GlideScope intubation in simulated difficult intubation: a randomized controlled study.","authors":"Ji Won Bak, Yeonji Noh, Juyoun Kim, Byeongmun Hwang, Seongsik Kang, Heejeong Son, Minsoo Kim","doi":"10.17085/apm.21095","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The GlideScope® videolaryngoscope (GVL) is widely used in patients with difficult airways and provides a good glottic view. However, the acute angle of the blade can make insertion and advancement of an endotracheal tube (ETT) more difficult than direct laryngoscopy, and the use of a stylet is recommended. This randomized controlled trial compared Parker Flex-It™ stylet (PFS) with GlideRite® rigid stylet (GRS) to facilitate intubation with the GVL in simulated difficult intubations.</p><p><strong>Methods: </strong>Fifty-four patients were randomly allocated to undergo GVL intubation using either GRS (GRS group) or PFS (PFS group). The total intubation time (TIT), 100-mm visual analog scale (VAS) for ease of intubation, success rate at the first attempt, use of laryngeal manipulation, tube advancement rate by assistant, and complications were recorded.</p><p><strong>Results: </strong>There was no significant difference between the GRS and PFS groups regarding TIT (50.3 ± 12.0 s in the GRS group and 57.8 ± 18.8 s in the PFS group, P = 0.108). However, intubation was more difficult in the PFS group than in the GRS group according to VAS score (P = 0.011). Cases in which the ETT was advanced from the stylet by an assistant, were more frequent in the GRS group than in the PFS group (P = 0.002). The overall incidence of possible complications was not significantly different.</p><p><strong>Conclusions: </strong>In patients with a simulated difficult airway, there was no difference in TIT using either the PFS or GRS. However, endotracheal intubation with PFS is more difficult to perform than GRS.</p>","PeriodicalId":7801,"journal":{"name":"Anesthesia and pain medicine","volume":"17 1","pages":"104-111"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/5a/apm-21095.PMC8841254.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.21095","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
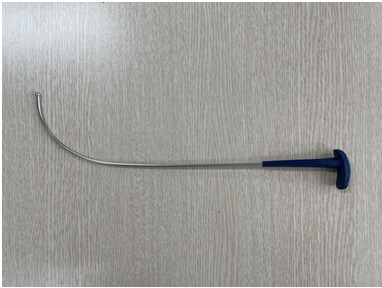
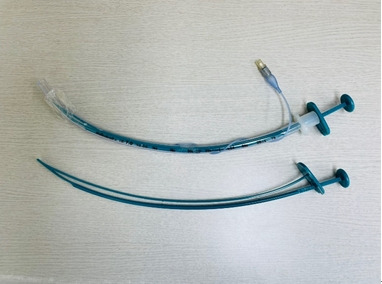
Background: The GlideScope® videolaryngoscope (GVL) is widely used in patients with difficult airways and provides a good glottic view. However, the acute angle of the blade can make insertion and advancement of an endotracheal tube (ETT) more difficult than direct laryngoscopy, and the use of a stylet is recommended. This randomized controlled trial compared Parker Flex-It™ stylet (PFS) with GlideRite® rigid stylet (GRS) to facilitate intubation with the GVL in simulated difficult intubations.
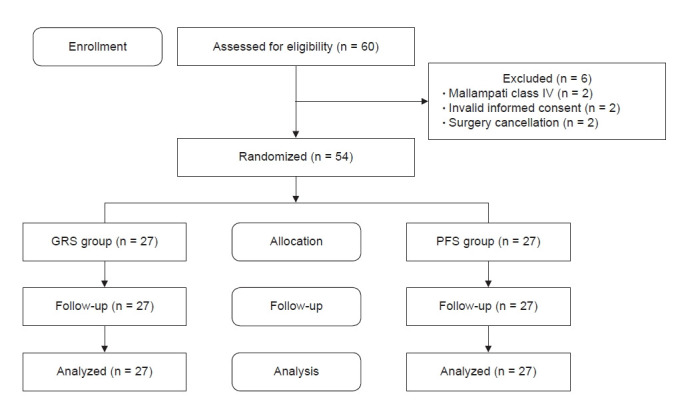
Methods: Fifty-four patients were randomly allocated to undergo GVL intubation using either GRS (GRS group) or PFS (PFS group). The total intubation time (TIT), 100-mm visual analog scale (VAS) for ease of intubation, success rate at the first attempt, use of laryngeal manipulation, tube advancement rate by assistant, and complications were recorded.
Results: There was no significant difference between the GRS and PFS groups regarding TIT (50.3 ± 12.0 s in the GRS group and 57.8 ± 18.8 s in the PFS group, P = 0.108). However, intubation was more difficult in the PFS group than in the GRS group according to VAS score (P = 0.011). Cases in which the ETT was advanced from the stylet by an assistant, were more frequent in the GRS group than in the PFS group (P = 0.002). The overall incidence of possible complications was not significantly different.
Conclusions: In patients with a simulated difficult airway, there was no difference in TIT using either the PFS or GRS. However, endotracheal intubation with PFS is more difficult to perform than GRS.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
