Ipek Gurol-Urganci, Lara Waite, Kirstin Webster, Jennifer Jardine, Fran Carroll, George Dunn, Alissa Frémeaux, Tina Harris, Jane Hawdon, Patrick Muller, Jan van der Meulen, Asma Khalil
{"title":"Obstetric interventions and pregnancy outcomes during the COVID-19 pandemic in England: A nationwide cohort study.","authors":"Ipek Gurol-Urganci, Lara Waite, Kirstin Webster, Jennifer Jardine, Fran Carroll, George Dunn, Alissa Frémeaux, Tina Harris, Jane Hawdon, Patrick Muller, Jan van der Meulen, Asma Khalil","doi":"10.1371/journal.pmed.1003884","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The COVID-19 pandemic has disrupted maternity services worldwide and imposed restrictions on societal behaviours. This national study aimed to compare obstetric intervention and pregnancy outcome rates in England during the pandemic and corresponding pre-pandemic calendar periods, and to assess whether differences in these rates varied according to ethnic and socioeconomic background.</p><p><strong>Methods and findings: </strong>We conducted a national study of singleton births in English National Health Service hospitals. We compared births during the COVID-19 pandemic period (23 March 2020 to 22 February 2021) with births during the corresponding calendar period 1 year earlier. The Hospital Episode Statistics database provided administrative hospital data about maternal characteristics, obstetric inventions (induction of labour, elective or emergency cesarean section, and instrumental birth), and outcomes (stillbirth, preterm birth, small for gestational age [SGA; birthweight < 10th centile], prolonged maternal length of stay (≥3 days), and maternal 42-day readmission). Multi-level logistic regression models were used to compare intervention and outcome rates between the corresponding pre-pandemic and pandemic calendar periods and to test for interactions between pandemic period and ethnic and socioeconomic background. All models were adjusted for maternal characteristics including age, obstetric history, comorbidities, and COVID-19 status at birth. The study included 948,020 singleton births (maternal characteristics: median age 30 years, 41.6% primiparous, 8.3% with gestational diabetes, 2.4% with preeclampsia, and 1.6% with pre-existing diabetes or hypertension); 451,727 births occurred during the defined pandemic period. Maternal characteristics were similar in the pre-pandemic and pandemic periods. Compared to the pre-pandemic period, stillbirth rates remained similar (0.36% pandemic versus 0.37% pre-pandemic, p = 0.16). Preterm birth and SGA birth rates were slightly lower during the pandemic (6.0% versus 6.1% for preterm births, adjusted odds ratio [aOR] 0.96, 95% CI 0.94-0.97; 5.6% versus 5.8% for SGA births, aOR 0.95, 95% CI 0.93-0.96; both p < 0.001). Slightly higher rates of obstetric intervention were observed during the pandemic (40.4% versus 39.1% for induction of labour, aOR 1.04, 95% CI 1.03-1.05; 13.9% versus 12.9% for elective cesarean section, aOR 1.13, 95% CI 1.11-1.14; 18.4% versus 17.0% for emergency cesarean section, aOR 1.07, 95% CI 1.06-1.08; all p < 0.001). Lower rates of prolonged maternal length of stay (16.7% versus 20.2%, aOR 0.77, 95% CI 0.76-0.78, p < 0.001) and maternal readmission (3.0% versus 3.3%, aOR 0.88, 95% CI 0.86-0.90, p < 0.001) were observed during the pandemic period. There was some evidence that differences in the rates of preterm birth, emergency cesarean section, and unassisted vaginal birth varied according to the mother's ethnic background but not according to her socioeconomic background. A key limitation is that multiple comparisons were made, increasing the chance of false-positive results.</p><p><strong>Conclusions: </strong>In this study, we found very small decreases in preterm birth and SGA birth rates and very small increases in induction of labour and elective and emergency cesarean section during the COVID-19 pandemic, with some evidence of a slightly different pattern of results in women from ethnic minority backgrounds. These changes in obstetric intervention rates and pregnancy outcomes may be linked to women's behaviour, environmental exposure, changes in maternity practice, or reduced staffing levels.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 1","pages":"e1003884"},"PeriodicalIF":9.9000,"publicationDate":"2022-01-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8803187/pdf/","citationCount":"31","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003884","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 31
Abstract
Background: The COVID-19 pandemic has disrupted maternity services worldwide and imposed restrictions on societal behaviours. This national study aimed to compare obstetric intervention and pregnancy outcome rates in England during the pandemic and corresponding pre-pandemic calendar periods, and to assess whether differences in these rates varied according to ethnic and socioeconomic background.
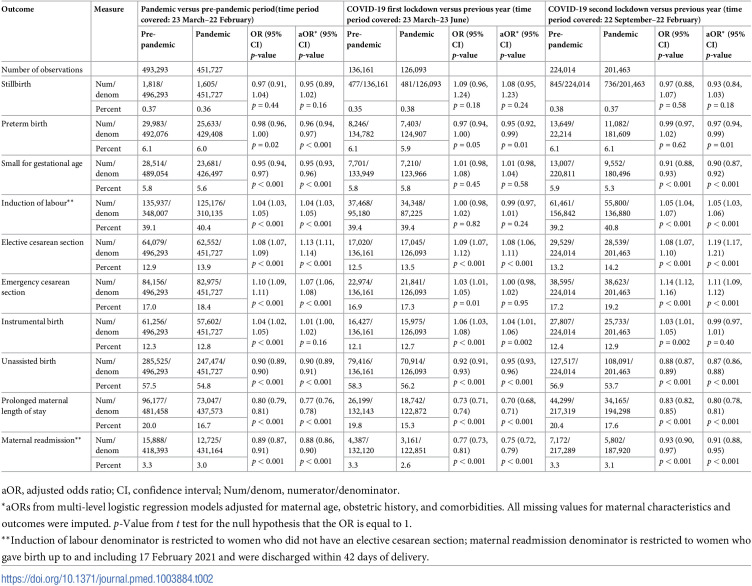
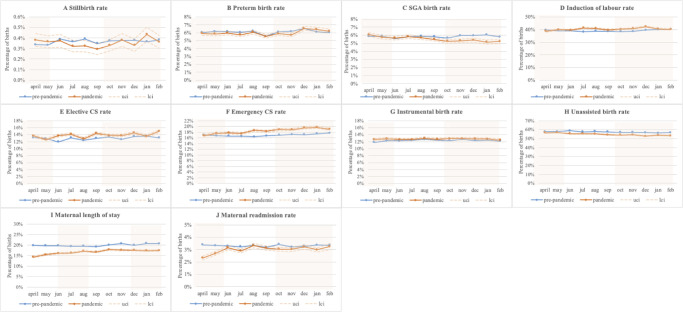
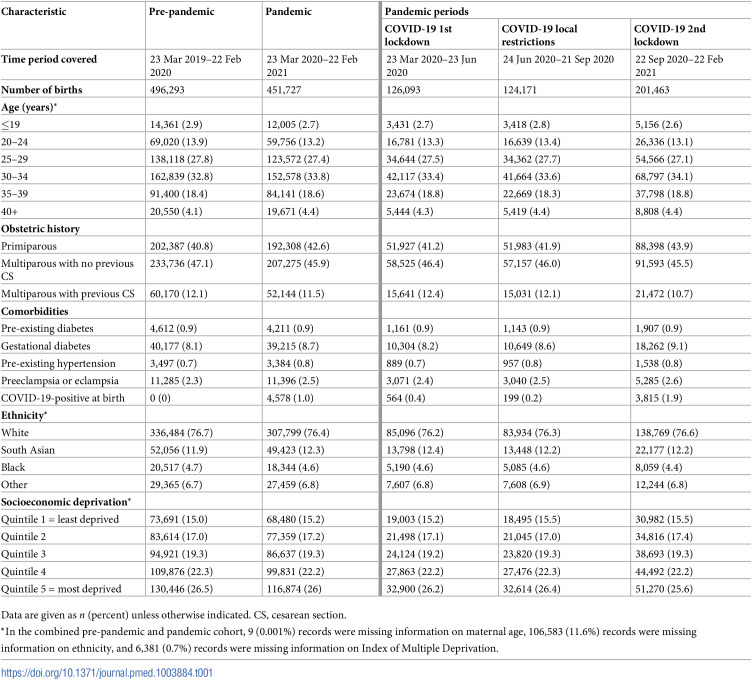
Methods and findings: We conducted a national study of singleton births in English National Health Service hospitals. We compared births during the COVID-19 pandemic period (23 March 2020 to 22 February 2021) with births during the corresponding calendar period 1 year earlier. The Hospital Episode Statistics database provided administrative hospital data about maternal characteristics, obstetric inventions (induction of labour, elective or emergency cesarean section, and instrumental birth), and outcomes (stillbirth, preterm birth, small for gestational age [SGA; birthweight < 10th centile], prolonged maternal length of stay (≥3 days), and maternal 42-day readmission). Multi-level logistic regression models were used to compare intervention and outcome rates between the corresponding pre-pandemic and pandemic calendar periods and to test for interactions between pandemic period and ethnic and socioeconomic background. All models were adjusted for maternal characteristics including age, obstetric history, comorbidities, and COVID-19 status at birth. The study included 948,020 singleton births (maternal characteristics: median age 30 years, 41.6% primiparous, 8.3% with gestational diabetes, 2.4% with preeclampsia, and 1.6% with pre-existing diabetes or hypertension); 451,727 births occurred during the defined pandemic period. Maternal characteristics were similar in the pre-pandemic and pandemic periods. Compared to the pre-pandemic period, stillbirth rates remained similar (0.36% pandemic versus 0.37% pre-pandemic, p = 0.16). Preterm birth and SGA birth rates were slightly lower during the pandemic (6.0% versus 6.1% for preterm births, adjusted odds ratio [aOR] 0.96, 95% CI 0.94-0.97; 5.6% versus 5.8% for SGA births, aOR 0.95, 95% CI 0.93-0.96; both p < 0.001). Slightly higher rates of obstetric intervention were observed during the pandemic (40.4% versus 39.1% for induction of labour, aOR 1.04, 95% CI 1.03-1.05; 13.9% versus 12.9% for elective cesarean section, aOR 1.13, 95% CI 1.11-1.14; 18.4% versus 17.0% for emergency cesarean section, aOR 1.07, 95% CI 1.06-1.08; all p < 0.001). Lower rates of prolonged maternal length of stay (16.7% versus 20.2%, aOR 0.77, 95% CI 0.76-0.78, p < 0.001) and maternal readmission (3.0% versus 3.3%, aOR 0.88, 95% CI 0.86-0.90, p < 0.001) were observed during the pandemic period. There was some evidence that differences in the rates of preterm birth, emergency cesarean section, and unassisted vaginal birth varied according to the mother's ethnic background but not according to her socioeconomic background. A key limitation is that multiple comparisons were made, increasing the chance of false-positive results.
Conclusions: In this study, we found very small decreases in preterm birth and SGA birth rates and very small increases in induction of labour and elective and emergency cesarean section during the COVID-19 pandemic, with some evidence of a slightly different pattern of results in women from ethnic minority backgrounds. These changes in obstetric intervention rates and pregnancy outcomes may be linked to women's behaviour, environmental exposure, changes in maternity practice, or reduced staffing levels.
背景:COVID-19大流行扰乱了世界各地的孕产妇服务,并对社会行为施加了限制。这项全国性研究旨在比较英格兰在大流行期间和相应的大流行前日历期间的产科干预和妊娠结局率,并评估这些比率的差异是否因种族和社会经济背景而异。方法和发现:我们对英国国家卫生服务医院的单胎分娩进行了一项全国性研究。我们将COVID-19大流行期间(2020年3月23日至2021年2月22日)的出生情况与一年前相应日历期间的出生情况进行了比较。医院事件统计数据库提供了有关产妇特征、产科发明(引产、选择性或紧急剖宫产和器械分娩)和结局(死胎、早产、小于胎龄)的医院行政数据[SGA;出生体重< 10百分位],产妇住院时间延长(≥3天),产妇再入院42天)。采用多级逻辑回归模型比较相应的大流行前和大流行日历期间的干预和结果率,并检验大流行期间与种族和社会经济背景之间的相互作用。所有模型都根据产妇特征进行了调整,包括年龄、产科史、合并症和出生时的COVID-19状况。该研究纳入948,020例单胎分娩(产妇特征:中位年龄30岁,41.6%为初产,8.3%患有妊娠期糖尿病,2.4%患有先兆子痫,1.6%患有糖尿病或高血压);在确定的大流行病期间,有451,727名婴儿出生。大流行前和大流行时期的产妇特征相似。与大流行前相比,死产率保持相似(大流行前0.36%与大流行前0.37%,p = 0.16)。大流行期间早产和SGA出生率略低(早产6.0% vs 6.1%,调整优势比[aOR] 0.96, 95% CI 0.94-0.97;SGA出生5.6% vs 5.8%, aOR 0.95, 95% CI 0.93-0.96;p均< 0.001)。大流行期间观察到的产科干预率略高(40.4%对39.1%的引产,aOR 1.04, 95% CI 1.03-1.05;择期剖宫产13.9% vs 12.9%, aOR 1.13, 95% CI 1.11-1.14;18.4%对17.0%急诊剖宫产,aOR 1.07, 95% CI 1.06-1.08;均p < 0.001)。在大流行期间,产妇延长住院时间的比率较低(16.7%对20.2%,aOR 0.77, 95% CI 0.76-0.78, p < 0.001)和产妇再入院率(3.0%对3.3%,aOR 0.88, 95% CI 0.86-0.90, p < 0.001)。有一些证据表明,早产率、紧急剖宫产率和无辅助阴道分娩率的差异因母亲的种族背景而异,但与她的社会经济背景无关。一个关键的限制是进行了多次比较,增加了假阳性结果的机会。结论:在本研究中,我们发现在COVID-19大流行期间,早产和SGA出生率的下降幅度很小,引产和选择性和紧急剖宫产的增加幅度很小,一些证据表明少数民族背景的妇女的结果模式略有不同。产科干预率和妊娠结局的这些变化可能与妇女的行为、环境暴露、产科实践的变化或人员配备水平的减少有关。
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
