Thomas Zheng Jie Teng, Jun Kiat Thaddaeus Tan, Samantha Baey, Sivaraj K Gunasekaran, Sameer P Junnarkar, Jee Keem Low, Cheong Wei Terence Huey, Vishal G Shelat
{"title":"Sequential organ failure assessment score is superior to other prognostic indices in acute pancreatitis.","authors":"Thomas Zheng Jie Teng, Jun Kiat Thaddaeus Tan, Samantha Baey, Sivaraj K Gunasekaran, Sameer P Junnarkar, Jee Keem Low, Cheong Wei Terence Huey, Vishal G Shelat","doi":"10.5492/wjccm.v10.i6.355","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute pancreatitis (AP) is a common surgical condition, with severe AP (SAP) potentially lethal. Many prognostic indices, including; acute physiology and chronic health evaluation II score (APACHE II), bedside index of severity in acute pancreatitis (BISAP), Glasgow score, harmless acute pancreatitis score (HAPS), Ranson's score, and sequential organ failure assessment (SOFA) evaluate AP severity and predict mortality.</p><p><strong>Aim: </strong>To evaluate these indices' utility in predicting severity, intensive care unit (ICU) admission, and mortality.</p><p><strong>Methods: </strong>A retrospective analysis of 653 patients with AP from July 2009 to September 2016 was performed. The demographic, clinical profile, and patient outcomes were collected. SAP was defined as <i>per</i> the revised Atlanta classification. Values for APACHE II score, BISAP, HAPS, and SOFA within 24 h of admission were retrospectively obtained based on laboratory results and patient evaluation recorded on a secure hospital-based online electronic platform. Data with < 10% missing data was imputed <i>via</i> mean substitution. Other patient information such as demographics, disease etiology, and patient outcomes were also derived from electronic medical records.</p><p><strong>Results: </strong>The mean age was 58.7 ± 17.5 years, with 58.7% males. Gallstones (<i>n</i> = 404, 61.9%), alcohol (<i>n</i> = 38, 5.8%), and hypertriglyceridemia (<i>n</i> = 19, 2.9%) were more common aetiologies. 81 (12.4%) patients developed SAP, 20 (3.1%) required ICU admission, and 12 (1.8%) deaths were attributed to SAP. Ranson's score and APACHE-II demonstrated the highest sensitivity in predicting SAP (92.6%, 80.2% respectively), ICU admission (100%), and mortality (100%). While SOFA and BISAP demonstrated lowest sensitivity in predicting SAP (13.6%, 24.7% respectively), ICU admission (40.0%, 25.0% respectively) and mortality (50.0%, 25.5% respectively). However, SOFA demonstrated the highest specificity in predicting SAP (99.7%), ICU admission (99.2%), and mortality (98.9%). SOFA demonstrated the highest positive predictive value, positive likelihood ratio, diagnostic odds ratio, and overall accuracy in predicting SAP, ICU admission, and mortality. SOFA and Ranson's score demonstrated the highest area under receiver-operator curves at 48 h in predicting SAP (0.966, 0.857 respectively), ICU admission (0.943, 0.946 respectively), and mortality (0.968, 0.917 respectively).</p><p><strong>Conclusion: </strong>The SOFA and 48-h Ranson's scores accurately predict severity, ICU admission, and mortality in AP, with more favorable statistics for the SOFA score.</p>","PeriodicalId":66959,"journal":{"name":"世界危重病急救学杂志(英文版)","volume":"10 6","pages":"355-368"},"PeriodicalIF":0.0000,"publicationDate":"2021-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/de/WJCCM-10-355.PMC8613719.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界危重病急救学杂志(英文版)","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5492/wjccm.v10.i6.355","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute pancreatitis (AP) is a common surgical condition, with severe AP (SAP) potentially lethal. Many prognostic indices, including; acute physiology and chronic health evaluation II score (APACHE II), bedside index of severity in acute pancreatitis (BISAP), Glasgow score, harmless acute pancreatitis score (HAPS), Ranson's score, and sequential organ failure assessment (SOFA) evaluate AP severity and predict mortality.
Aim: To evaluate these indices' utility in predicting severity, intensive care unit (ICU) admission, and mortality.
Methods: A retrospective analysis of 653 patients with AP from July 2009 to September 2016 was performed. The demographic, clinical profile, and patient outcomes were collected. SAP was defined as per the revised Atlanta classification. Values for APACHE II score, BISAP, HAPS, and SOFA within 24 h of admission were retrospectively obtained based on laboratory results and patient evaluation recorded on a secure hospital-based online electronic platform. Data with < 10% missing data was imputed via mean substitution. Other patient information such as demographics, disease etiology, and patient outcomes were also derived from electronic medical records.
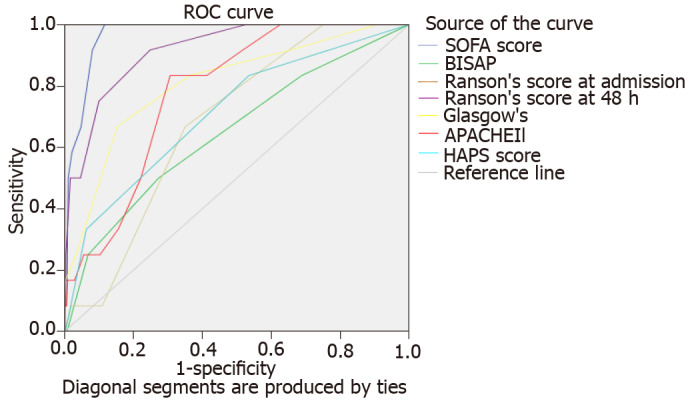
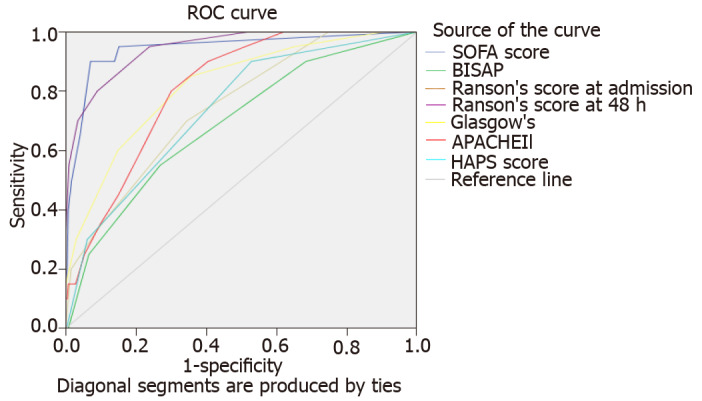
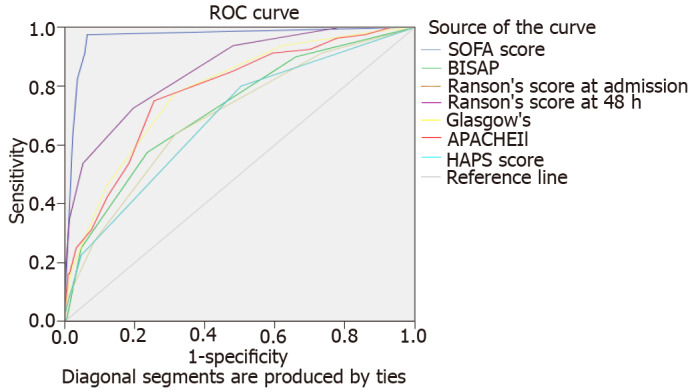
Results: The mean age was 58.7 ± 17.5 years, with 58.7% males. Gallstones (n = 404, 61.9%), alcohol (n = 38, 5.8%), and hypertriglyceridemia (n = 19, 2.9%) were more common aetiologies. 81 (12.4%) patients developed SAP, 20 (3.1%) required ICU admission, and 12 (1.8%) deaths were attributed to SAP. Ranson's score and APACHE-II demonstrated the highest sensitivity in predicting SAP (92.6%, 80.2% respectively), ICU admission (100%), and mortality (100%). While SOFA and BISAP demonstrated lowest sensitivity in predicting SAP (13.6%, 24.7% respectively), ICU admission (40.0%, 25.0% respectively) and mortality (50.0%, 25.5% respectively). However, SOFA demonstrated the highest specificity in predicting SAP (99.7%), ICU admission (99.2%), and mortality (98.9%). SOFA demonstrated the highest positive predictive value, positive likelihood ratio, diagnostic odds ratio, and overall accuracy in predicting SAP, ICU admission, and mortality. SOFA and Ranson's score demonstrated the highest area under receiver-operator curves at 48 h in predicting SAP (0.966, 0.857 respectively), ICU admission (0.943, 0.946 respectively), and mortality (0.968, 0.917 respectively).
Conclusion: The SOFA and 48-h Ranson's scores accurately predict severity, ICU admission, and mortality in AP, with more favorable statistics for the SOFA score.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
