Geert-Jan Geersing, Toshihiko Takada, Frederikus A Klok, Harry R Büller, D Mark Courtney, Yonathan Freund, Javier Galipienzo, Gregoire Le Gal, Waleed Ghanima, Jeffrey A Kline, Menno V Huisman, Karel G M Moons, Arnaud Perrier, Sameer Parpia, Helia Robert-Ebadi, Marc Righini, Pierre-Marie Roy, Maarten van Smeden, Milou A M Stals, Philip S Wells, Kerstin de Wit, Noémie Kraaijpoel, Nick van Es
{"title":"Ruling out pulmonary embolism across different healthcare settings: A systematic review and individual patient data meta-analysis.","authors":"Geert-Jan Geersing, Toshihiko Takada, Frederikus A Klok, Harry R Büller, D Mark Courtney, Yonathan Freund, Javier Galipienzo, Gregoire Le Gal, Waleed Ghanima, Jeffrey A Kline, Menno V Huisman, Karel G M Moons, Arnaud Perrier, Sameer Parpia, Helia Robert-Ebadi, Marc Righini, Pierre-Marie Roy, Maarten van Smeden, Milou A M Stals, Philip S Wells, Kerstin de Wit, Noémie Kraaijpoel, Nick van Es","doi":"10.1371/journal.pmed.1003905","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The challenging clinical dilemma of detecting pulmonary embolism (PE) in suspected patients is encountered in a variety of healthcare settings. We hypothesized that the optimal diagnostic approach to detect these patients in terms of safety and efficiency depends on underlying PE prevalence, case mix, and physician experience, overall reflected by the type of setting where patients are initially assessed. The objective of this study was to assess the capability of ruling out PE by available diagnostic strategies across all possible settings.</p><p><strong>Methods and findings: </strong>We performed a literature search (MEDLINE) followed by an individual patient data (IPD) meta-analysis (MA; 23 studies), including patients from self-referral emergency care (n = 12,612), primary healthcare clinics (n = 3,174), referred secondary care (n = 17,052), and hospitalized or nursing home patients (n = 2,410). Multilevel logistic regression was performed to evaluate diagnostic performance of the Wells and revised Geneva rules, both using fixed and adapted D-dimer thresholds to age or pretest probability (PTP), for the YEARS algorithm and for the Pulmonary Embolism Rule-out Criteria (PERC). All strategies were tested separately in each healthcare setting. Following studies done in this field, the primary diagnostic metrices estimated from the models were the \"failure rate\" of each strategy-i.e., the proportion of missed PE among patients categorized as \"PE excluded\" and \"efficiency\"-defined as the proportion of patients categorized as \"PE excluded\" among all patients. In self-referral emergency care, the PERC algorithm excludes PE in 21% of suspected patients at a failure rate of 1.12% (95% confidence interval [CI] 0.74 to 1.70), whereas this increases to 6.01% (4.09 to 8.75) in referred patients to secondary care at an efficiency of 10%. In patients from primary healthcare and those referred to secondary care, strategies adjusting D-dimer to PTP are the most efficient (range: 43% to 62%) at a failure rate ranging between 0.25% and 3.06%, with higher failure rates observed in patients referred to secondary care. For this latter setting, strategies adjusting D-dimer to age are associated with a lower failure rate ranging between 0.65% and 0.81%, yet are also less efficient (range: 33% and 35%). For all strategies, failure rates are highest in hospitalized or nursing home patients, ranging between 1.68% and 5.13%, at an efficiency ranging between 15% and 30%. The main limitation of the primary analyses was that the diagnostic performance of each strategy was compared in different sets of studies since the availability of items used in each diagnostic strategy differed across included studies; however, sensitivity analyses suggested that the findings were robust.</p><p><strong>Conclusions: </strong>The capability of safely and efficiently ruling out PE of available diagnostic strategies differs for different healthcare settings. The findings of this IPD MA help in determining the optimum diagnostic strategies for ruling out PE per healthcare setting, balancing the trade-off between failure rate and efficiency of each strategy.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 1","pages":"e1003905"},"PeriodicalIF":9.9000,"publicationDate":"2022-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8824365/pdf/","citationCount":"14","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003905","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 14
Abstract
Background: The challenging clinical dilemma of detecting pulmonary embolism (PE) in suspected patients is encountered in a variety of healthcare settings. We hypothesized that the optimal diagnostic approach to detect these patients in terms of safety and efficiency depends on underlying PE prevalence, case mix, and physician experience, overall reflected by the type of setting where patients are initially assessed. The objective of this study was to assess the capability of ruling out PE by available diagnostic strategies across all possible settings.
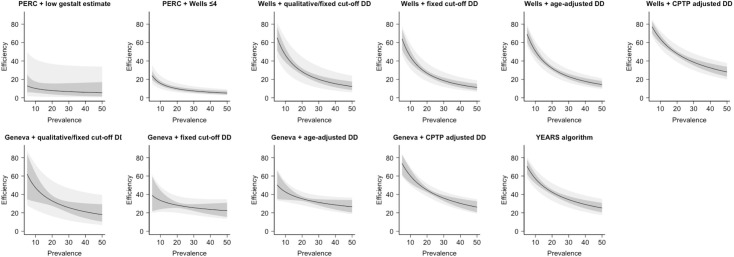
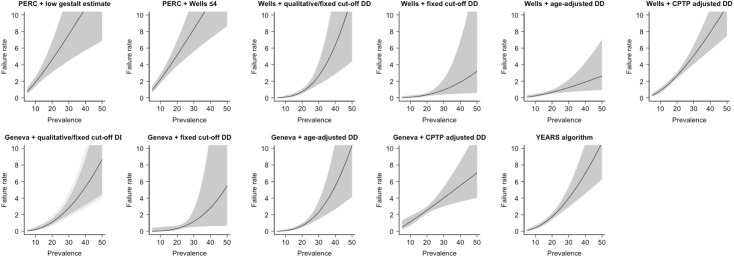
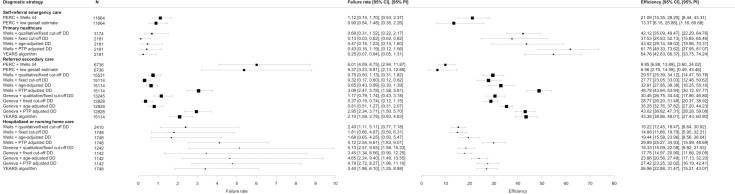
Methods and findings: We performed a literature search (MEDLINE) followed by an individual patient data (IPD) meta-analysis (MA; 23 studies), including patients from self-referral emergency care (n = 12,612), primary healthcare clinics (n = 3,174), referred secondary care (n = 17,052), and hospitalized or nursing home patients (n = 2,410). Multilevel logistic regression was performed to evaluate diagnostic performance of the Wells and revised Geneva rules, both using fixed and adapted D-dimer thresholds to age or pretest probability (PTP), for the YEARS algorithm and for the Pulmonary Embolism Rule-out Criteria (PERC). All strategies were tested separately in each healthcare setting. Following studies done in this field, the primary diagnostic metrices estimated from the models were the "failure rate" of each strategy-i.e., the proportion of missed PE among patients categorized as "PE excluded" and "efficiency"-defined as the proportion of patients categorized as "PE excluded" among all patients. In self-referral emergency care, the PERC algorithm excludes PE in 21% of suspected patients at a failure rate of 1.12% (95% confidence interval [CI] 0.74 to 1.70), whereas this increases to 6.01% (4.09 to 8.75) in referred patients to secondary care at an efficiency of 10%. In patients from primary healthcare and those referred to secondary care, strategies adjusting D-dimer to PTP are the most efficient (range: 43% to 62%) at a failure rate ranging between 0.25% and 3.06%, with higher failure rates observed in patients referred to secondary care. For this latter setting, strategies adjusting D-dimer to age are associated with a lower failure rate ranging between 0.65% and 0.81%, yet are also less efficient (range: 33% and 35%). For all strategies, failure rates are highest in hospitalized or nursing home patients, ranging between 1.68% and 5.13%, at an efficiency ranging between 15% and 30%. The main limitation of the primary analyses was that the diagnostic performance of each strategy was compared in different sets of studies since the availability of items used in each diagnostic strategy differed across included studies; however, sensitivity analyses suggested that the findings were robust.
Conclusions: The capability of safely and efficiently ruling out PE of available diagnostic strategies differs for different healthcare settings. The findings of this IPD MA help in determining the optimum diagnostic strategies for ruling out PE per healthcare setting, balancing the trade-off between failure rate and efficiency of each strategy.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
