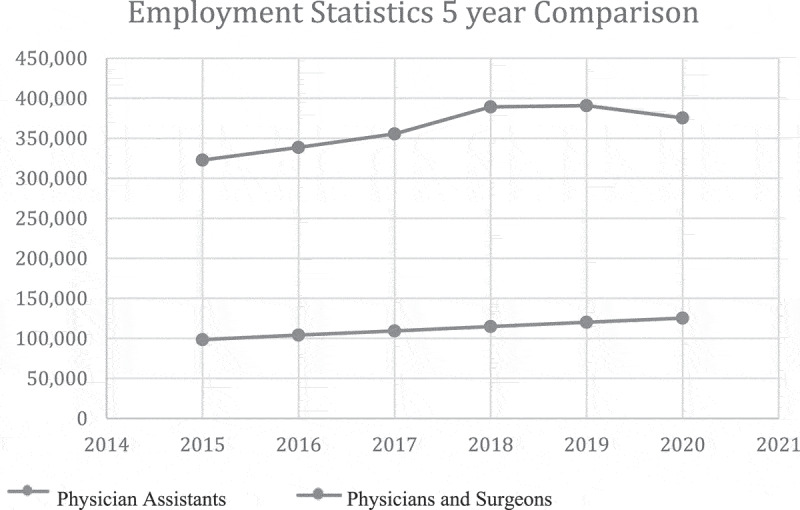
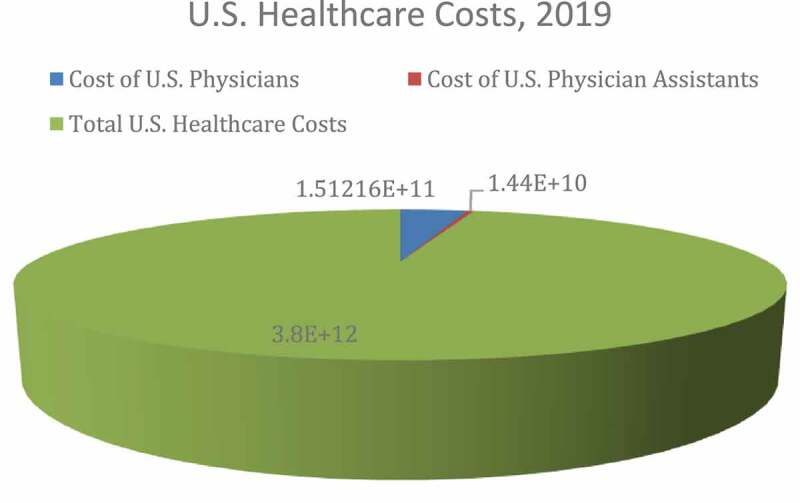
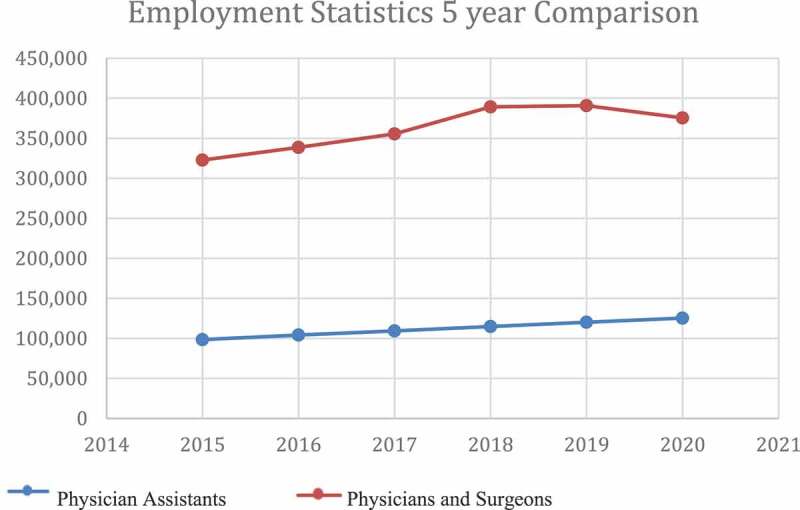
{"title":"Increased reliance on physician assistants: an access-quality tradeoff?","authors":"Bhavneet Walia, Harshdeep Banga, David A Larsen","doi":"10.1080/20016689.2022.2030559","DOIUrl":null,"url":null,"abstract":"Overview In recent years, Physician Assistants (PAs) have become an increasingly important class of medical practioners in the USA (U.S.) healthcare system. After physicians, PAs and Nurse Practitioners are the most skilled among the commonly observed types of medical practitioners, having earned a Masters Degree from an accredited medical sciences program. Further, PAs perform many of the same tasks as physicians within the U.S. healthcare system. According to the American Association of Physician Assistants, PAs commonly: ‘Take medical histories; Conduct physical exams; Diagnose and treat illness; Order and interpret tests; Develop treatment plans; Prescribe medication; Counsel on preventive care; Perform procedures; Assist in surgery; Make rounds in hospitals and nursing homes; Do clinical research.’ [1] These tasks can either be transferred from physicians to PAs or completed in physician-PA teams. As such, PAs can act as substitutes or complements for physicians within U.S. healthcare and other healthcare systems. More specifically, PAs can work without day-to-day physician supervision while performing physician-like tasks or in teams in which they are directly supervised by physicians [2]. Given that their tasks are highly related to those of U.S. physicians, it is important to characterize trends in the role and scale of PAs in the U.S. healthcare system. The number of PAs is growing at a rapid rate in U.S. healthcare systems [3]. The number of employed PAs in the U.S. is expected to grow by 39,300 or 31.3% between 2019 and 2029. This growth rate is well above the average rate of labor growth in the healthcare industry. By comparison, the projected growth rate for U.S. physician and surgeon positions over the same time period is 3.6%, with a projected 27,300 new physician/surgeon positions over that time. Figure 1 shows the beginning of this projected trend. These projections suggest that the ratio of physicians to PAs will decrease from 6:1 in 2019 to 4.7:1 in 2029. This rapid change can be linked to structural shifts in the U.S. healthcare systems, including increased demand attributable partly to the Affordable Care Act of 2010, an increased market concentration of for-profit health institutions that seek to maximize profit partly by reducing labor costs, and a fairly-substantial average pay gap between physicians and PAs, among others. Presently, we consider whether this shift will create a tradeoff between health care access and quality within U.S. healthcare. In 2019, median physician pay in the U.S. was $208,000 compared to $115,390 for Pas [3]. Consequently, the cost savings from increasing the proportion of PAs relative to physicians are substantial. The BLS projects that the number of U.S. PAs and physicians combined will expand to 944,500 by 2029. If this expansion were to be conducted while preserving the 6:1 physician-to-PA ratio observed in 2019, it would cost approximately $1.38 trillion more systemwide at current salaries, as calculated from the previous BLS data and assuming that the expansion is linear in time. In these worker categories, the respective workforces were approximately 727,000 for physicians and 125,000 for PAs in 2019 [3]. Therefore, the salary cost of U.S. physicians in that year was approximately $151.2 billion or 4.0% of total U.S. healthcare costs, and the salary cost of U.S. PAs was approximately $14.4 billion or 0.38% of total U.S. healthcare costs. While perhaps not a primary driver of healthcare cost in the U.S., physician personnel costs are substantial, both in dollar and percentage terms. Figure 2 visualizes the extent of these costs relative to overall U.S. healthcare costs.","PeriodicalId":73811,"journal":{"name":"Journal of market access & health policy","volume":"10 1","pages":"2030559"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/81/ZJMA_10_2030559.PMC8788342.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of market access & health policy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20016689.2022.2030559","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
Abstract
Overview In recent years, Physician Assistants (PAs) have become an increasingly important class of medical practioners in the USA (U.S.) healthcare system. After physicians, PAs and Nurse Practitioners are the most skilled among the commonly observed types of medical practitioners, having earned a Masters Degree from an accredited medical sciences program. Further, PAs perform many of the same tasks as physicians within the U.S. healthcare system. According to the American Association of Physician Assistants, PAs commonly: ‘Take medical histories; Conduct physical exams; Diagnose and treat illness; Order and interpret tests; Develop treatment plans; Prescribe medication; Counsel on preventive care; Perform procedures; Assist in surgery; Make rounds in hospitals and nursing homes; Do clinical research.’ [1] These tasks can either be transferred from physicians to PAs or completed in physician-PA teams. As such, PAs can act as substitutes or complements for physicians within U.S. healthcare and other healthcare systems. More specifically, PAs can work without day-to-day physician supervision while performing physician-like tasks or in teams in which they are directly supervised by physicians [2]. Given that their tasks are highly related to those of U.S. physicians, it is important to characterize trends in the role and scale of PAs in the U.S. healthcare system. The number of PAs is growing at a rapid rate in U.S. healthcare systems [3]. The number of employed PAs in the U.S. is expected to grow by 39,300 or 31.3% between 2019 and 2029. This growth rate is well above the average rate of labor growth in the healthcare industry. By comparison, the projected growth rate for U.S. physician and surgeon positions over the same time period is 3.6%, with a projected 27,300 new physician/surgeon positions over that time. Figure 1 shows the beginning of this projected trend. These projections suggest that the ratio of physicians to PAs will decrease from 6:1 in 2019 to 4.7:1 in 2029. This rapid change can be linked to structural shifts in the U.S. healthcare systems, including increased demand attributable partly to the Affordable Care Act of 2010, an increased market concentration of for-profit health institutions that seek to maximize profit partly by reducing labor costs, and a fairly-substantial average pay gap between physicians and PAs, among others. Presently, we consider whether this shift will create a tradeoff between health care access and quality within U.S. healthcare. In 2019, median physician pay in the U.S. was $208,000 compared to $115,390 for Pas [3]. Consequently, the cost savings from increasing the proportion of PAs relative to physicians are substantial. The BLS projects that the number of U.S. PAs and physicians combined will expand to 944,500 by 2029. If this expansion were to be conducted while preserving the 6:1 physician-to-PA ratio observed in 2019, it would cost approximately $1.38 trillion more systemwide at current salaries, as calculated from the previous BLS data and assuming that the expansion is linear in time. In these worker categories, the respective workforces were approximately 727,000 for physicians and 125,000 for PAs in 2019 [3]. Therefore, the salary cost of U.S. physicians in that year was approximately $151.2 billion or 4.0% of total U.S. healthcare costs, and the salary cost of U.S. PAs was approximately $14.4 billion or 0.38% of total U.S. healthcare costs. While perhaps not a primary driver of healthcare cost in the U.S., physician personnel costs are substantial, both in dollar and percentage terms. Figure 2 visualizes the extent of these costs relative to overall U.S. healthcare costs.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
