Evaluation of Short-Term Outcomes and the Learning Curve Wherein a Thoracic Resident Doctor Performed Video-Assisted Thoracoscopic Anatomical Lung Resection for Lung Cancer.
{"title":"Evaluation of Short-Term Outcomes and the Learning Curve Wherein a Thoracic Resident Doctor Performed Video-Assisted Thoracoscopic Anatomical Lung Resection for Lung Cancer.","authors":"Tomohiro Fujita, Shigeyuki Morino, Akihiro Nakamura","doi":"10.5761/atcs.oa.21-00216","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The surgical approach for anatomical lung resection includes open thoracotomy, video-assisted thoracoscopic surgery, and robot-assisted thoracoscopic surgery. We evaluated the short-term outcomes and the learning curve wherein a thoracic resident doctor consecutively performed video-assisted thoracoscopic anatomical lung resection for lung cancer.</p><p><strong>Methods: </strong>We retrospectively reviewed 91 cases of consecutive video-assisted thoracoscopic anatomical lung resections for lung cancer performed by a thoracic resident doctor between November 2017 and March 2020. The thoracic resident doctor had no previous experience performing video-assisted thoracoscopic or open anatomical lung resection.</p><p><strong>Results: </strong>Lobectomy was performed in 80 cases. Simple segmentectomy was performed in 11 cases. No cases required intraoperative conversion to open thoracotomy. The median operative time and blood loss were 148 min and 10 ml, respectively. There were no serious postoperative complications or deaths 30 days after surgery. The learning curve was examined using the cumulative sum method with operative time as a factor, and it took 21 cases to attain experience.</p><p><strong>Conclusion: </strong>Our resident doctor safely performed video-assisted thoracoscopic anatomical lung resections and it took 21 cases to stabilize the surgical technique. The surgical technique was possibly stabilized earlier than previously reported, although this was a study of a single resident doctor.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"28 4","pages":"249-254"},"PeriodicalIF":1.3000,"publicationDate":"2022-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/26/a3/atcs-28-249.PMC9433889.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.21-00216","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The surgical approach for anatomical lung resection includes open thoracotomy, video-assisted thoracoscopic surgery, and robot-assisted thoracoscopic surgery. We evaluated the short-term outcomes and the learning curve wherein a thoracic resident doctor consecutively performed video-assisted thoracoscopic anatomical lung resection for lung cancer.
Methods: We retrospectively reviewed 91 cases of consecutive video-assisted thoracoscopic anatomical lung resections for lung cancer performed by a thoracic resident doctor between November 2017 and March 2020. The thoracic resident doctor had no previous experience performing video-assisted thoracoscopic or open anatomical lung resection.
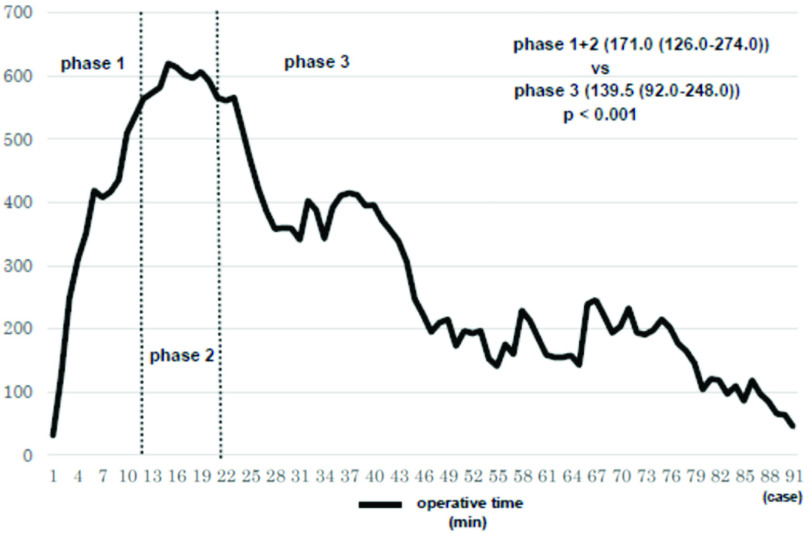
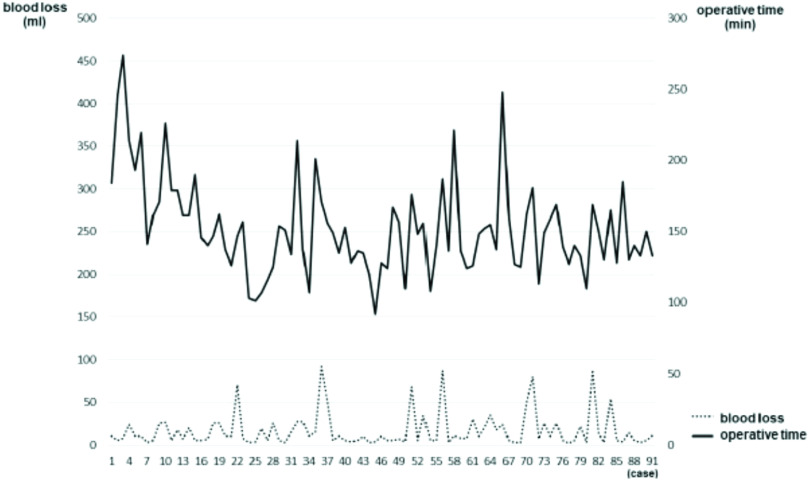
Results: Lobectomy was performed in 80 cases. Simple segmentectomy was performed in 11 cases. No cases required intraoperative conversion to open thoracotomy. The median operative time and blood loss were 148 min and 10 ml, respectively. There were no serious postoperative complications or deaths 30 days after surgery. The learning curve was examined using the cumulative sum method with operative time as a factor, and it took 21 cases to attain experience.
Conclusion: Our resident doctor safely performed video-assisted thoracoscopic anatomical lung resections and it took 21 cases to stabilize the surgical technique. The surgical technique was possibly stabilized earlier than previously reported, although this was a study of a single resident doctor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
