Antidepressant discontinuation before or during pregnancy and risk of psychiatric emergency in Denmark: A population-based propensity score-matched cohort study.
{"title":"Antidepressant discontinuation before or during pregnancy and risk of psychiatric emergency in Denmark: A population-based propensity score-matched cohort study.","authors":"Xiaoqin Liu, Nina Molenaar, Esben Agerbo, Natalie C Momen, Anna-Sophie Rommel, Angela Lupattelli, Veerle Bergink, Trine Munk-Olsen","doi":"10.1371/journal.pmed.1003895","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Women prescribed antidepressants face the dilemma of whether or not to continue their treatment during pregnancy. Currently, limited evidence is available on the efficacy of continuing versus discontinuing antidepressant treatment during pregnancy to aid their decision. We aimed to estimate whether antidepressant discontinuation before or during pregnancy was associated with an increased risk of psychiatric emergency (ascertained by psychiatric admission or emergency room visit), a proxy measure of severe exacerbation of symptoms/mental health crisis.</p><p><strong>Methods and findings: </strong>We carried out a propensity score-matched cohort study of women who gave birth to live-born singletons between January 1, 1997 and June 30, 2016 in Denmark and who redeemed an antidepressant prescription in the 90 days before the pregnancy, identified by Anatomical Therapeutic Chemical (ATC) code N06A. We constructed 2 matched cohorts, matching each woman who discontinued antidepressants before pregnancy (N = 2,669) or during pregnancy (N = 5,467) to one who continued antidepressants based on propensity scores. Maternal characteristics and variables related to disease severity were used to generate the propensity scores in logistic regression models. We estimated hazard ratios (HRs) of psychiatric emergency in the perinatal period (pregnancy and 6 months postpartum) using stratified Cox regression. Psychiatric emergencies were observed in 76 women who discontinued antidepressants before pregnancy and 91 women who continued. There was no evidence of higher risk of psychiatric emergency among women who discontinued antidepressants before pregnancy (cumulative incidence: 2.9%, 95% confidence interval [CI]: 2.3% to 3.6% for discontinuation versus 3.4%, 95% CI: 2.8% to 4.2% for continuation; HR = 0.84, 95% CI: 0.61 to 1.16, p = 0.298). Overall, 202 women who discontinued antidepressants during pregnancy and 156 who continued had psychiatric emergencies (cumulative incidence: 5.0%, 95% CI: 4.2% to 5.9% versus 3.7%, 95% CI: 3.1% to 4.5%). Antidepressant discontinuation during pregnancy was associated with increased risk of psychiatric emergency (HR = 1.25, 95% CI: 1.00 to 1.55, p = 0.048). Study limitations include lack of information on indications for antidepressant treatment and reasons for discontinuing antidepressants.</p><p><strong>Conclusions: </strong>In this study, we found that discontinuing antidepressant medication during pregnancy (but not before) is associated with an apparent increased risk of psychiatric emergency compared to continuing treatment throughout pregnancy.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 1","pages":"e1003895"},"PeriodicalIF":9.9000,"publicationDate":"2022-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8843130/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003895","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Women prescribed antidepressants face the dilemma of whether or not to continue their treatment during pregnancy. Currently, limited evidence is available on the efficacy of continuing versus discontinuing antidepressant treatment during pregnancy to aid their decision. We aimed to estimate whether antidepressant discontinuation before or during pregnancy was associated with an increased risk of psychiatric emergency (ascertained by psychiatric admission or emergency room visit), a proxy measure of severe exacerbation of symptoms/mental health crisis.
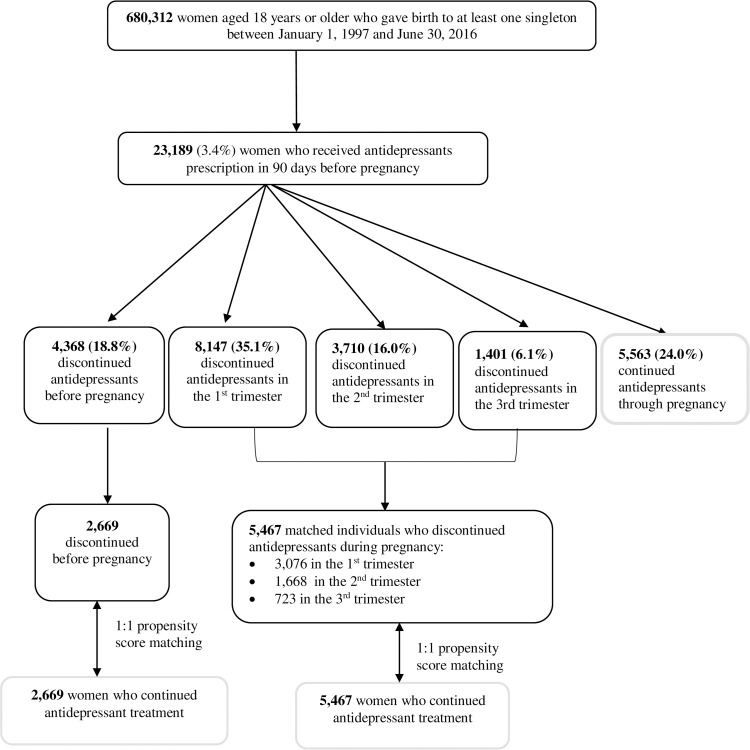
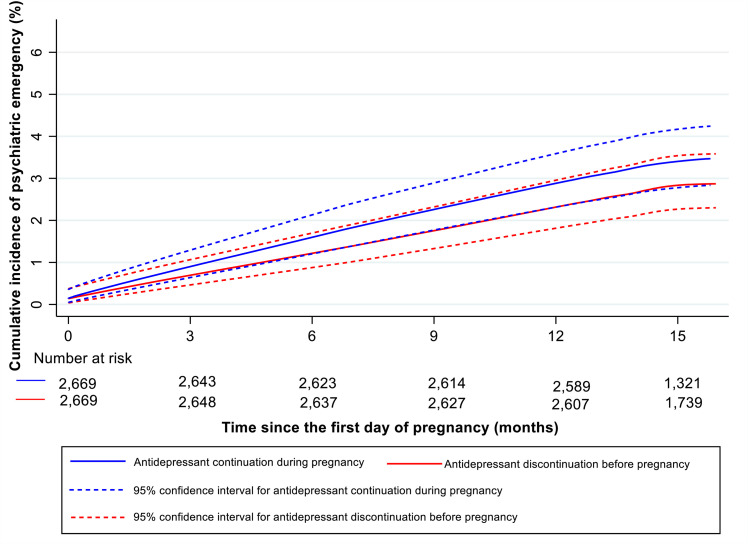
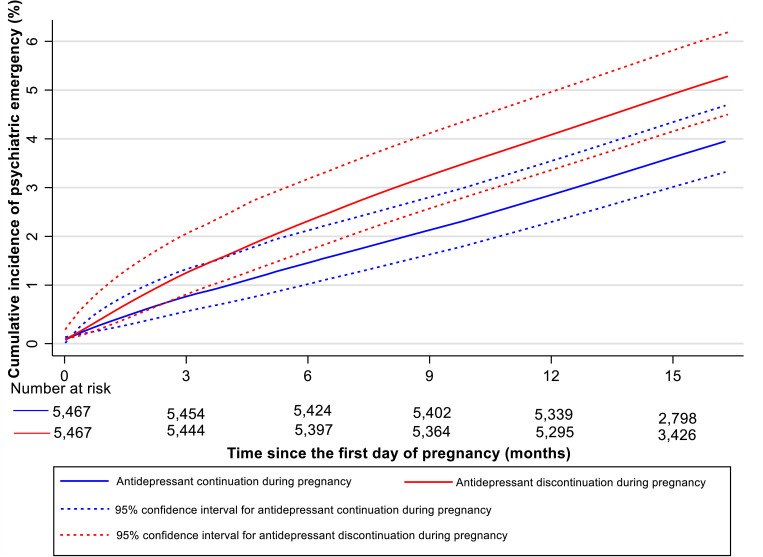
Methods and findings: We carried out a propensity score-matched cohort study of women who gave birth to live-born singletons between January 1, 1997 and June 30, 2016 in Denmark and who redeemed an antidepressant prescription in the 90 days before the pregnancy, identified by Anatomical Therapeutic Chemical (ATC) code N06A. We constructed 2 matched cohorts, matching each woman who discontinued antidepressants before pregnancy (N = 2,669) or during pregnancy (N = 5,467) to one who continued antidepressants based on propensity scores. Maternal characteristics and variables related to disease severity were used to generate the propensity scores in logistic regression models. We estimated hazard ratios (HRs) of psychiatric emergency in the perinatal period (pregnancy and 6 months postpartum) using stratified Cox regression. Psychiatric emergencies were observed in 76 women who discontinued antidepressants before pregnancy and 91 women who continued. There was no evidence of higher risk of psychiatric emergency among women who discontinued antidepressants before pregnancy (cumulative incidence: 2.9%, 95% confidence interval [CI]: 2.3% to 3.6% for discontinuation versus 3.4%, 95% CI: 2.8% to 4.2% for continuation; HR = 0.84, 95% CI: 0.61 to 1.16, p = 0.298). Overall, 202 women who discontinued antidepressants during pregnancy and 156 who continued had psychiatric emergencies (cumulative incidence: 5.0%, 95% CI: 4.2% to 5.9% versus 3.7%, 95% CI: 3.1% to 4.5%). Antidepressant discontinuation during pregnancy was associated with increased risk of psychiatric emergency (HR = 1.25, 95% CI: 1.00 to 1.55, p = 0.048). Study limitations include lack of information on indications for antidepressant treatment and reasons for discontinuing antidepressants.
Conclusions: In this study, we found that discontinuing antidepressant medication during pregnancy (but not before) is associated with an apparent increased risk of psychiatric emergency compared to continuing treatment throughout pregnancy.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
