Appropriate determination of the surgical transepicondylar axis can be achieved following distal femur resection in navigation-assisted total knee arthroplasty.
Sang Jun Song, Hyun Woo Lee, Kang Il Kim, Cheol Hee Park
{"title":"Appropriate determination of the surgical transepicondylar axis can be achieved following distal femur resection in navigation-assisted total knee arthroplasty.","authors":"Sang Jun Song, Hyun Woo Lee, Kang Il Kim, Cheol Hee Park","doi":"10.1186/s43019-021-00123-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Many surgeons have determined the surgical transepicondylar axis (sTEA) after distal femur resection in total knee arthroplasty (TKA). However, in most navigation systems, the registration of the sTEA precedes the distal femur resection. This sequential difference can influence the accuracy of intraoperative determination for sTEA when considering the proximal location of the anatomical references for sTEA and the arthritic environment. We compared the accuracy and precision in determinations of the sTEA between before and after distal femur resection during navigation-assisted TKA.</p><p><strong>Methods: </strong>Ninety TKAs with Attune posterior-stabilized prostheses were performed under imageless navigation. The sTEA was registered before distal femur resection, then reassessed and adjusted after distal resection. The femoral component was implanted finally according to the sTEA determined after distal femur resection. Computed tomography (CT) was performed postoperatively to analyze the true sTEA (the line connecting the tip of the lateral femoral epicondyle to the lowest point of the medial femoral epicondylar sulcus on axial CT images) and femoral component rotation (FCR) axis. The FCR angle after distal femur resection (FCRA-aR) was defined as the angle between the FCR axis and true sTEA on CT images. The FCR angle before distal resection (FCRA-bR) could be presumed to be the value of FCRA-aR minus the difference between the intraoperatively determined sTEAs before and after distal resection as indicated by the navigation system. It was considered that the FCRA-bR or FCRA-aR represented the differences between the sTEA determined before or after distal femur resection and the true sTEA, respectively.</p><p><strong>Results: </strong>The FCRA-bR was -1.3 ± 2.4° and FCRA-aR was 0.3 ± 1.7° (p < 0.001). The range of FCRA-bR was from -6.6° to 4.1° and that of FCRA-aR was from -2.7° to 3.3°. The proportion of appropriate FCRA (≤ ±3°) was significantly higher after distal femur resection than that before resection (91.1% versus 70%; p < 0.001).</p><p><strong>Conclusions: </strong>The FCR was more appropriate when the sTEA was determined after distal femur resection than before resection in navigation-assisted TKA. The reassessment and adjusted registration of sTEA after distal femur resection could improve the rotational alignment of the femoral component in navigation-assisted TKA.</p><p><strong>Level of evidence: </strong>IV.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":"33 1","pages":"41"},"PeriodicalIF":4.4000,"publicationDate":"2021-11-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8579642/pdf/","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-021-00123-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 9
Abstract
Background: Many surgeons have determined the surgical transepicondylar axis (sTEA) after distal femur resection in total knee arthroplasty (TKA). However, in most navigation systems, the registration of the sTEA precedes the distal femur resection. This sequential difference can influence the accuracy of intraoperative determination for sTEA when considering the proximal location of the anatomical references for sTEA and the arthritic environment. We compared the accuracy and precision in determinations of the sTEA between before and after distal femur resection during navigation-assisted TKA.
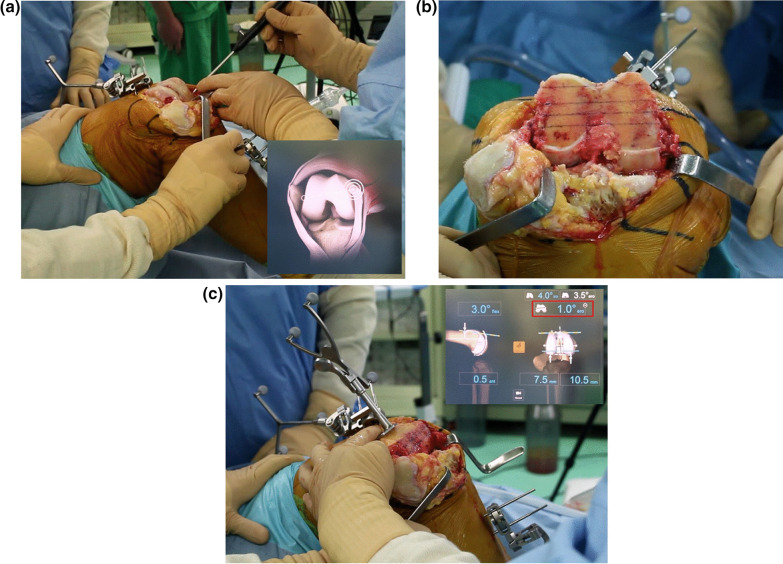
Methods: Ninety TKAs with Attune posterior-stabilized prostheses were performed under imageless navigation. The sTEA was registered before distal femur resection, then reassessed and adjusted after distal resection. The femoral component was implanted finally according to the sTEA determined after distal femur resection. Computed tomography (CT) was performed postoperatively to analyze the true sTEA (the line connecting the tip of the lateral femoral epicondyle to the lowest point of the medial femoral epicondylar sulcus on axial CT images) and femoral component rotation (FCR) axis. The FCR angle after distal femur resection (FCRA-aR) was defined as the angle between the FCR axis and true sTEA on CT images. The FCR angle before distal resection (FCRA-bR) could be presumed to be the value of FCRA-aR minus the difference between the intraoperatively determined sTEAs before and after distal resection as indicated by the navigation system. It was considered that the FCRA-bR or FCRA-aR represented the differences between the sTEA determined before or after distal femur resection and the true sTEA, respectively.
Results: The FCRA-bR was -1.3 ± 2.4° and FCRA-aR was 0.3 ± 1.7° (p < 0.001). The range of FCRA-bR was from -6.6° to 4.1° and that of FCRA-aR was from -2.7° to 3.3°. The proportion of appropriate FCRA (≤ ±3°) was significantly higher after distal femur resection than that before resection (91.1% versus 70%; p < 0.001).
Conclusions: The FCR was more appropriate when the sTEA was determined after distal femur resection than before resection in navigation-assisted TKA. The reassessment and adjusted registration of sTEA after distal femur resection could improve the rotational alignment of the femoral component in navigation-assisted TKA.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
