{"title":"Comparison of radiation exposure and clinical outcomes between transradial and transfemoral diagnostic cerebral approaches: a retrospective study.","authors":"Curtis Amankwah, Lauren Lombardo, John Rutledge, Ahsan Sattar, Bree Chancellor, Dorothea Altschul","doi":"10.1136/bmjsit-2021-000110","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To identify and compare patient and procedural variables that are associated with a high radiation dose exposure and worse clinical outcomes between transradial arterial (TRA) and transfemoral arterial (TFA) approaches.</p><p><strong>Design: </strong>This was a retrospective analysis.</p><p><strong>Setting: </strong>A community hospital during the initial phase of adopting a TRA-first approach.</p><p><strong>Participants: </strong>A resultant 215 subjects who only underwent diagnostic cerebral angiograms (DCA) after excluding all therapeutic procedures and patients under 18 years.</p><p><strong>Interventions: </strong>Only DCA from 1 May 2018 to 31 January 2021.</p><p><strong>Main outcome measures: </strong>We compared radiation exposure parameters (total fluoroscopy time (FT), total radiation dose (TD) and dose area product (DAP), number of vessels injected and Patient-Reported Global Health Physical and Mental Outcome Scores (PROGHS) at 30 days postprocedure between groups.</p><p><strong>Results: </strong>FT was significantly greater in TRA compared with TFA (p<0.001). In addition, TRA had a significantly higher TD (p=0.002) and DAP (p=0.005) when compared with TFA. Analysis of only 6-vessel DCAs also showed that TRA had a significantly higher FT, DAP and TD in comparison to TFA. Despite observing a longer FT in TRA, results showed fewer vessels injected and a notably lower success rate in acquiring a 6-vessel DCA using the TRA. Further analysis of the effect of vessel number on FT using general linear models showed that with every increase of one vessel, the FT increases by 2.2 min for TRA (p<0.001; 95% CI 1.03 to 3.36) and by 1.3 min for TFA (p<0.001; 95% CI 0.72 to 1.83). There was no significant difference between groups in PROGHS mental and physical t-scores at 30 days postprocedure, even though our cohort showed a significantly greater percentage of TRA procedures done in the outpatient setting.</p><p><strong>Conclusions: </strong>Adopting a TRA first approach for DCAs may be initially associated with a higher radiation dose for the patient. Better strategies and devices are needed to mitigate this effect.</p>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":" ","pages":"e000110"},"PeriodicalIF":4.7000,"publicationDate":"2022-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/d5/bmjsit-2021-000110.PMC8785198.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2021-000110","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To identify and compare patient and procedural variables that are associated with a high radiation dose exposure and worse clinical outcomes between transradial arterial (TRA) and transfemoral arterial (TFA) approaches.
Design: This was a retrospective analysis.
Setting: A community hospital during the initial phase of adopting a TRA-first approach.
Participants: A resultant 215 subjects who only underwent diagnostic cerebral angiograms (DCA) after excluding all therapeutic procedures and patients under 18 years.
Interventions: Only DCA from 1 May 2018 to 31 January 2021.
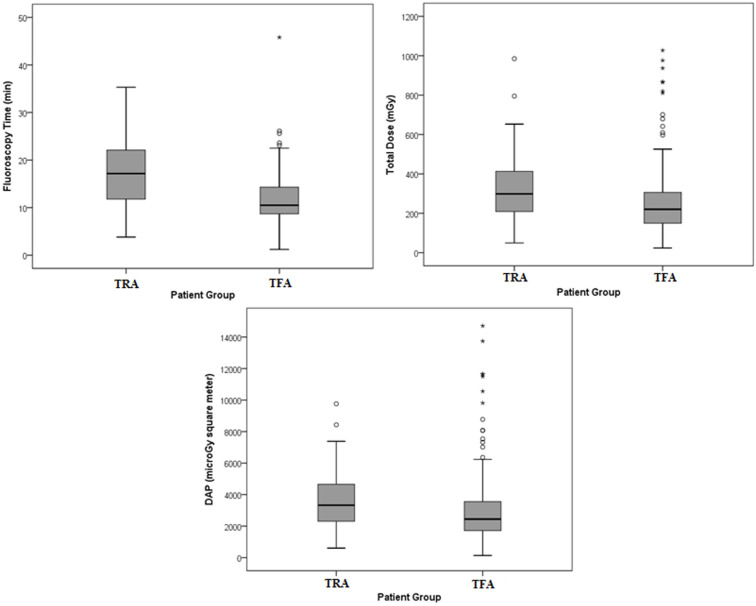
Main outcome measures: We compared radiation exposure parameters (total fluoroscopy time (FT), total radiation dose (TD) and dose area product (DAP), number of vessels injected and Patient-Reported Global Health Physical and Mental Outcome Scores (PROGHS) at 30 days postprocedure between groups.
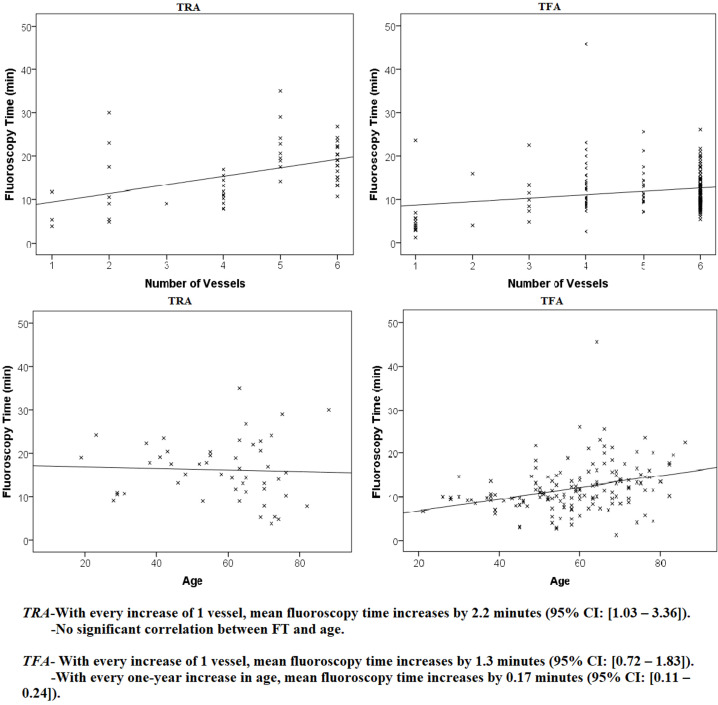
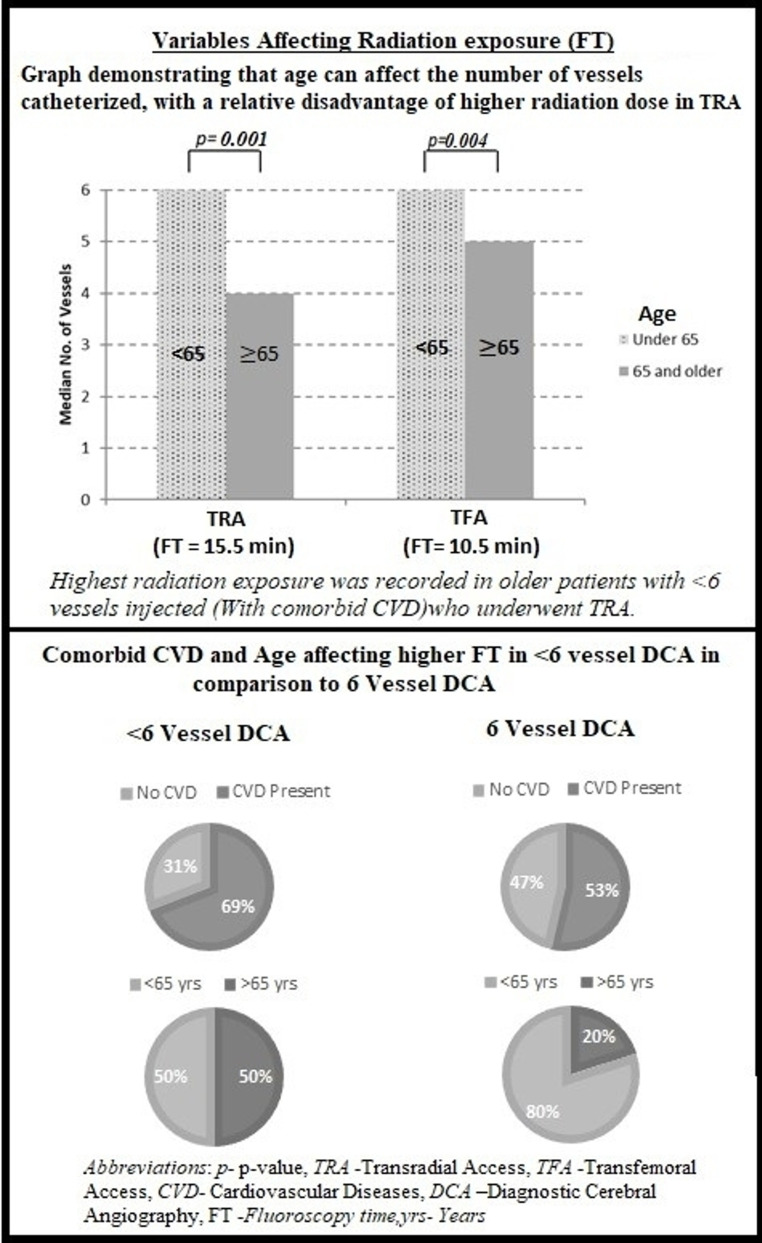
Results: FT was significantly greater in TRA compared with TFA (p<0.001). In addition, TRA had a significantly higher TD (p=0.002) and DAP (p=0.005) when compared with TFA. Analysis of only 6-vessel DCAs also showed that TRA had a significantly higher FT, DAP and TD in comparison to TFA. Despite observing a longer FT in TRA, results showed fewer vessels injected and a notably lower success rate in acquiring a 6-vessel DCA using the TRA. Further analysis of the effect of vessel number on FT using general linear models showed that with every increase of one vessel, the FT increases by 2.2 min for TRA (p<0.001; 95% CI 1.03 to 3.36) and by 1.3 min for TFA (p<0.001; 95% CI 0.72 to 1.83). There was no significant difference between groups in PROGHS mental and physical t-scores at 30 days postprocedure, even though our cohort showed a significantly greater percentage of TRA procedures done in the outpatient setting.
Conclusions: Adopting a TRA first approach for DCAs may be initially associated with a higher radiation dose for the patient. Better strategies and devices are needed to mitigate this effect.
目的确定并比较经桡动脉(TRA)和经股动脉(TFA)方法中与高辐射剂量暴露和较差临床结果相关的患者和手术变量:设计:这是一项回顾性分析:环境: 一家社区医院,在采用 TRA 优先方法的初始阶段:在排除所有治疗程序和 18 岁以下患者后,215 名受试者仅接受了诊断性脑血管造影(DCA):主要结果测量:我们比较了各组间的辐射暴露参数(总透视时间(FT)、总辐射剂量(TD)和剂量面积乘积(DAP)、注射血管数量以及术后30天患者报告的全球健康身心结果评分(PROGHS):结果:与 TFA 相比,TRA 的 FT 明显更高(p结论:采用 TRA 为先的方法进行大动脉造影术,可大大提高手术的成功率:在 DCA 中首先采用 TRA 方法,最初可能会给患者带来较高的辐射剂量。需要更好的策略和设备来减轻这种影响。
期刊介绍:
ACS Applied Bio Materials is an interdisciplinary journal publishing original research covering all aspects of biomaterials and biointerfaces including and beyond the traditional biosensing, biomedical and therapeutic applications.
The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrates knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important bio applications. The journal is specifically interested in work that addresses the relationship between structure and function and assesses the stability and degradation of materials under relevant environmental and biological conditions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
