Monetary incentives and peer referral in promoting secondary distribution of HIV self-testing among men who have sex with men in China: A randomized controlled trial.
Yi Zhou, Ying Lu, Yuxin Ni, Dan Wu, Xi He, Jason J Ong, Joseph D Tucker, Sean Y Sylvia, Fengshi Jing, Xiaofeng Li, Shanzi Huang, Guangquan Shen, Chen Xu, Yuan Xiong, Yongjie Sha, Mengyuan Cheng, Junjie Xu, Hongbo Jiang, Wencan Dai, Liqun Huang, Fei Zou, Cheng Wang, Bin Yang, Wenhua Mei, Weiming Tang
{"title":"Monetary incentives and peer referral in promoting secondary distribution of HIV self-testing among men who have sex with men in China: A randomized controlled trial.","authors":"Yi Zhou, Ying Lu, Yuxin Ni, Dan Wu, Xi He, Jason J Ong, Joseph D Tucker, Sean Y Sylvia, Fengshi Jing, Xiaofeng Li, Shanzi Huang, Guangquan Shen, Chen Xu, Yuan Xiong, Yongjie Sha, Mengyuan Cheng, Junjie Xu, Hongbo Jiang, Wencan Dai, Liqun Huang, Fei Zou, Cheng Wang, Bin Yang, Wenhua Mei, Weiming Tang","doi":"10.1371/journal.pmed.1003928","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Digital network-based methods may enhance peer distribution of HIV self-testing (HIVST) kits, but interventions that can optimize this approach are needed. We aimed to assess whether monetary incentives and peer referral could improve a secondary distribution program for HIVST among men who have sex with men (MSM) in China.</p><p><strong>Methods and findings: </strong>Between October 21, 2019 and September 14, 2020, a 3-arm randomized controlled, single-blinded trial was conducted online among 309 individuals (defined as index participants) who were assigned male at birth, aged 18 years or older, ever had male-to-male sex, willing to order HIVST kits online, and consented to take surveys online. We randomly assigned index participants into one of the 3 arms: (1) standard secondary distribution (control) group (n = 102); (2) secondary distribution with monetary incentives (SD-M) group (n = 103); and (3) secondary distribution with monetary incentives plus peer referral (SD-M-PR) group (n = 104). Index participants in 3 groups were encouraged to order HIVST kits online and distribute to members within their social networks. Members who received kits directly from index participants or through peer referral links from index MSM were defined as alters. Index participants in the 2 intervention groups could receive a fixed incentive ($3 USD) online for the verified test result uploaded to the digital platform by each unique alter. Index participants in the SD-M-PR group could additionally have a personalized peer referral link for alters to order kits online. Both index participants and alters needed to pay a refundable deposit ($15 USD) for ordering a kit. All index participants were assigned an online 3-month follow-up survey after ordering kits. The primary outcomes were the mean number of alters motivated by index participants in each arm and the mean number of newly tested alters motivated by index participants in each arm. These were assessed using zero-inflated negative binomial regression to determine the group differences in the mean number of alters and the mean number of newly tested alters motivated by index participants. Analyses were performed on an intention-to-treat basis. We also conducted an economic evaluation using microcosting from a health provider perspective with a 3-month time horizon. The mean number of unique tested alters motivated by index participants was 0.57 ± 0.96 (mean ± standard deviation [SD]) in the control group, compared with 0.98 ± 1.38 in the SD-M group (mean difference [MD] = 0.41),and 1.78 ± 2.05 in the SD-M-PR group (MD = 1.21). The mean number of newly tested alters motivated by index participants was 0.16 ± 0.39 (mean ± SD) in the control group, compared with 0.41 ± 0.73 in the SD-M group (MD = 0.25) and 0.57 ± 0.91 in the SD-M-PR group (MD = 0.41), respectively. Results indicated that index participants in intervention arms were more likely to motivate unique tested alters (control versus SD-M: incidence rate ratio [IRR = 2.98, 95% CI = 1.82 to 4.89, p-value < 0.001; control versus SD-M-PR: IRR = 3.26, 95% CI = 2.29 to 4.63, p-value < 0.001) and newly tested alters (control versus SD-M: IRR = 4.22, 95% CI = 1.93 to 9.23, p-value < 0.001; control versus SD-M-PR: IRR = 3.49, 95% CI = 1.92 to 6.37, p-value < 0.001) to conduct HIVST. The proportion of newly tested testers among alters was 28% in the control group, 42% in the SD-M group, and 32% in the SD-M-PR group. A total of 18 testers (3 index participants and 15 alters) tested as HIV positive, and the HIV reactive rates for alters were similar between the 3 groups. The total costs were $19,485.97 for 794 testers, including 450 index participants and 344 alter testers. Overall, the average cost per tester was $24.54, and the average cost per alter tester was $56.65. Monetary incentives alone (SD-M group) were more cost-effective than monetary incentives with peer referral (SD-M-PR group) on average in terms of alters tested and newly tested alters, despite SD-M-PR having larger effects. Compared to the control group, the cost for one more alter tester in the SD-M group was $14.90 and $16.61 in the SD-M-PR group. For newly tested alters, the cost of one more alter in the SD-M group was $24.65 and $49.07 in the SD-M-PR group. No study-related adverse events were reported during the study. Limitations include the digital network approach might neglect individuals who lack internet access.</p><p><strong>Conclusions: </strong>Monetary incentives alone and the combined intervention of monetary incentives and peer referral can promote the secondary distribution of HIVST among MSM. Monetary incentives can also expand HIV testing by encouraging first-time testing through secondary distribution by MSM. This social network-based digital approach can be expanded to other public health research, especially in the era of the Coronavirus Disease 2019 (COVID-19).</p><p><strong>Trial registration: </strong>Chinese Clinical Trial Registry (ChiCTR) ChiCTR1900025433.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 2","pages":"e1003928"},"PeriodicalIF":9.9000,"publicationDate":"2022-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8887971/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1003928","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Digital network-based methods may enhance peer distribution of HIV self-testing (HIVST) kits, but interventions that can optimize this approach are needed. We aimed to assess whether monetary incentives and peer referral could improve a secondary distribution program for HIVST among men who have sex with men (MSM) in China.
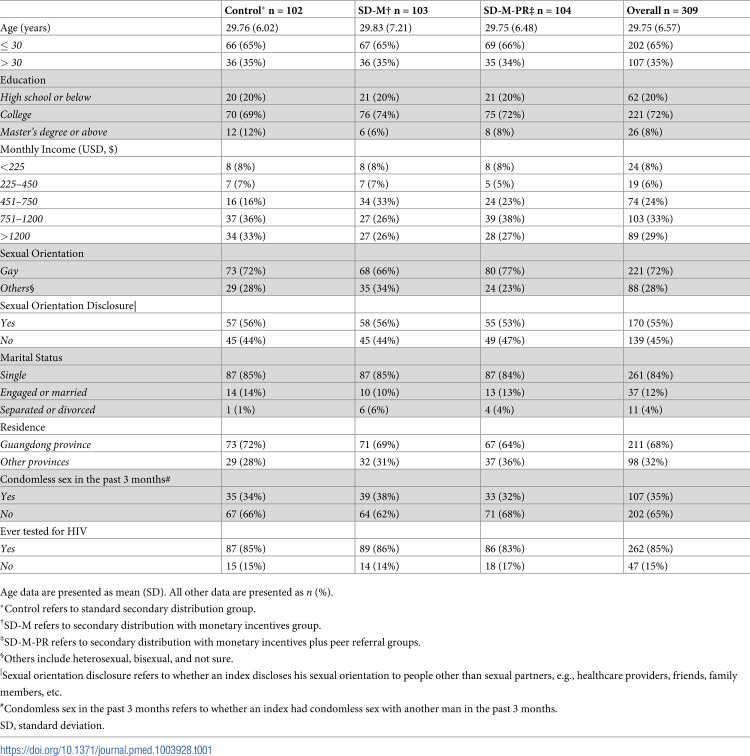
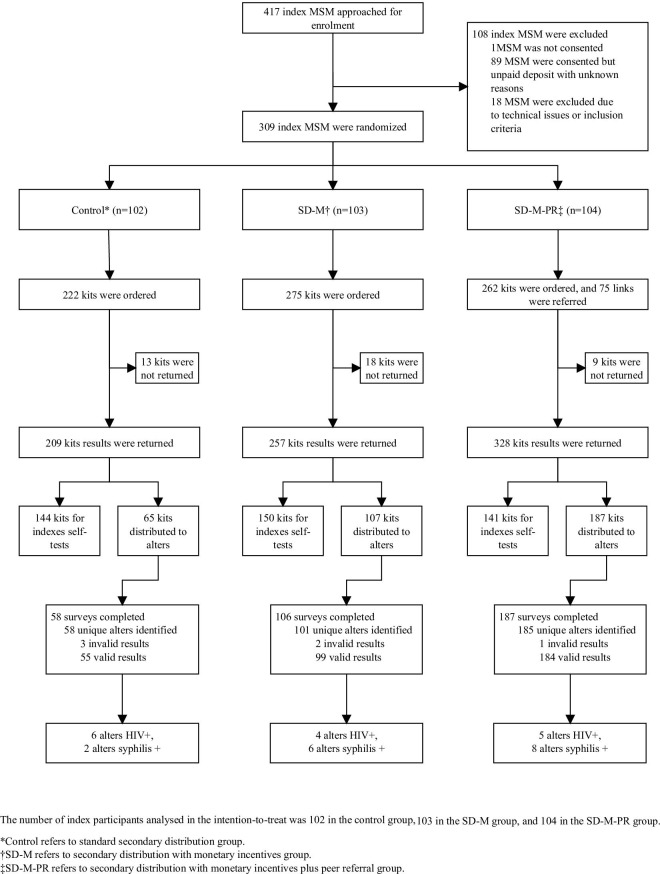
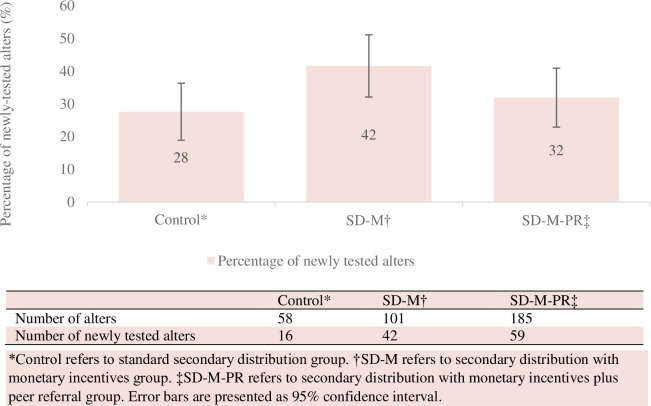
Methods and findings: Between October 21, 2019 and September 14, 2020, a 3-arm randomized controlled, single-blinded trial was conducted online among 309 individuals (defined as index participants) who were assigned male at birth, aged 18 years or older, ever had male-to-male sex, willing to order HIVST kits online, and consented to take surveys online. We randomly assigned index participants into one of the 3 arms: (1) standard secondary distribution (control) group (n = 102); (2) secondary distribution with monetary incentives (SD-M) group (n = 103); and (3) secondary distribution with monetary incentives plus peer referral (SD-M-PR) group (n = 104). Index participants in 3 groups were encouraged to order HIVST kits online and distribute to members within their social networks. Members who received kits directly from index participants or through peer referral links from index MSM were defined as alters. Index participants in the 2 intervention groups could receive a fixed incentive ($3 USD) online for the verified test result uploaded to the digital platform by each unique alter. Index participants in the SD-M-PR group could additionally have a personalized peer referral link for alters to order kits online. Both index participants and alters needed to pay a refundable deposit ($15 USD) for ordering a kit. All index participants were assigned an online 3-month follow-up survey after ordering kits. The primary outcomes were the mean number of alters motivated by index participants in each arm and the mean number of newly tested alters motivated by index participants in each arm. These were assessed using zero-inflated negative binomial regression to determine the group differences in the mean number of alters and the mean number of newly tested alters motivated by index participants. Analyses were performed on an intention-to-treat basis. We also conducted an economic evaluation using microcosting from a health provider perspective with a 3-month time horizon. The mean number of unique tested alters motivated by index participants was 0.57 ± 0.96 (mean ± standard deviation [SD]) in the control group, compared with 0.98 ± 1.38 in the SD-M group (mean difference [MD] = 0.41),and 1.78 ± 2.05 in the SD-M-PR group (MD = 1.21). The mean number of newly tested alters motivated by index participants was 0.16 ± 0.39 (mean ± SD) in the control group, compared with 0.41 ± 0.73 in the SD-M group (MD = 0.25) and 0.57 ± 0.91 in the SD-M-PR group (MD = 0.41), respectively. Results indicated that index participants in intervention arms were more likely to motivate unique tested alters (control versus SD-M: incidence rate ratio [IRR = 2.98, 95% CI = 1.82 to 4.89, p-value < 0.001; control versus SD-M-PR: IRR = 3.26, 95% CI = 2.29 to 4.63, p-value < 0.001) and newly tested alters (control versus SD-M: IRR = 4.22, 95% CI = 1.93 to 9.23, p-value < 0.001; control versus SD-M-PR: IRR = 3.49, 95% CI = 1.92 to 6.37, p-value < 0.001) to conduct HIVST. The proportion of newly tested testers among alters was 28% in the control group, 42% in the SD-M group, and 32% in the SD-M-PR group. A total of 18 testers (3 index participants and 15 alters) tested as HIV positive, and the HIV reactive rates for alters were similar between the 3 groups. The total costs were $19,485.97 for 794 testers, including 450 index participants and 344 alter testers. Overall, the average cost per tester was $24.54, and the average cost per alter tester was $56.65. Monetary incentives alone (SD-M group) were more cost-effective than monetary incentives with peer referral (SD-M-PR group) on average in terms of alters tested and newly tested alters, despite SD-M-PR having larger effects. Compared to the control group, the cost for one more alter tester in the SD-M group was $14.90 and $16.61 in the SD-M-PR group. For newly tested alters, the cost of one more alter in the SD-M group was $24.65 and $49.07 in the SD-M-PR group. No study-related adverse events were reported during the study. Limitations include the digital network approach might neglect individuals who lack internet access.
Conclusions: Monetary incentives alone and the combined intervention of monetary incentives and peer referral can promote the secondary distribution of HIVST among MSM. Monetary incentives can also expand HIV testing by encouraging first-time testing through secondary distribution by MSM. This social network-based digital approach can be expanded to other public health research, especially in the era of the Coronavirus Disease 2019 (COVID-19).
Trial registration: Chinese Clinical Trial Registry (ChiCTR) ChiCTR1900025433.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
