{"title":"Isolated oculomotor nerve palsy secondary to non-aneurysmal subarachnoid hemorrhage.","authors":"Shyle Mehta, Abhijith Bathini, Anwesha Dubey, Awinita Barpujari, Ahmad Kassem, Mohanad Sulaiman, Mandy Binning","doi":"10.7461/jcen.2022.E2021.06.007","DOIUrl":null,"url":null,"abstract":"<p><p>We present a case series of two patients who developed unilateral cranial nerve III (CNIII) palsy following non-aneurysmal SAH (NASAH). Subarachnoid hemorrhage (SAH) can present with various signs and symptoms. Early diagnosis is paramount to determine treatment course. Thus, clinicians must be aware of the variable clinical presentations of this condition. Two patients were admitted to a single institution for SAH. Patient 1, 52-year-old male, presented with headache, left eye ptosis, and painless diplopia. A non-contrast head computed tomography (CT) demonstrated a SAH within the left sylvian fissure and blood surrounding the mesencephalon and falx. Patient 2, 70-year-old male, presented with mild headache, acute onset of blurry vision, and right eye ptosis. A non-contrast head CT demonstrated a diffuse SAH predominantly in the Sylvian and suprasellar cisterns. Patients were admitted to the neuro intensive care unit and underwent diagnostic angiograms to identify possible aneurysms. Magnetic resonance imaging and angiograms for both patients were negative. Patients were managed with best medical therapy and followed up in the outpatient setting. Unilateral CNIII palsy in the setting of NASAH was identified in both patients. Diagnostic angiograms were negative for aneurysms; therefore, SAH were determined to be spontaneous. We propose that unilateral CNIII palsy is a possible sign of NASAH.</p>","PeriodicalId":15359,"journal":{"name":"Journal of Cerebrovascular and Endovascular Neurosurgery","volume":" ","pages":"267-275"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/96/b9/jcen-2022-e2021-06-007.PMC9537643.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cerebrovascular and Endovascular Neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7461/jcen.2022.E2021.06.007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/3/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
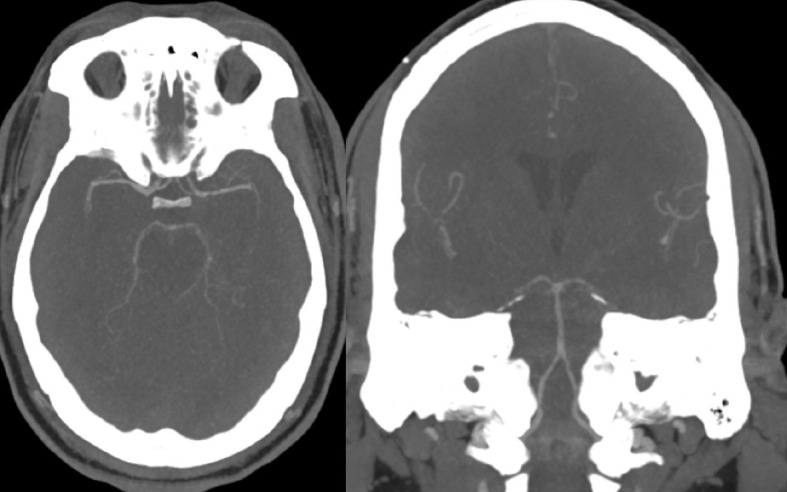
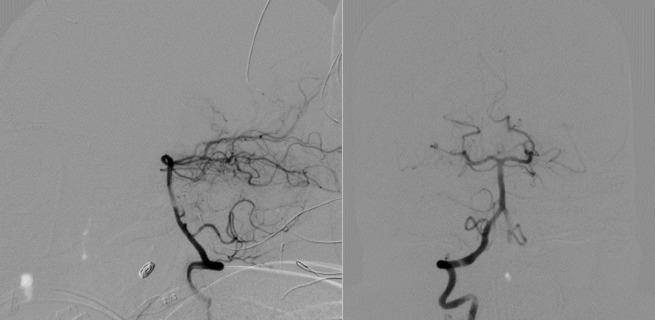
We present a case series of two patients who developed unilateral cranial nerve III (CNIII) palsy following non-aneurysmal SAH (NASAH). Subarachnoid hemorrhage (SAH) can present with various signs and symptoms. Early diagnosis is paramount to determine treatment course. Thus, clinicians must be aware of the variable clinical presentations of this condition. Two patients were admitted to a single institution for SAH. Patient 1, 52-year-old male, presented with headache, left eye ptosis, and painless diplopia. A non-contrast head computed tomography (CT) demonstrated a SAH within the left sylvian fissure and blood surrounding the mesencephalon and falx. Patient 2, 70-year-old male, presented with mild headache, acute onset of blurry vision, and right eye ptosis. A non-contrast head CT demonstrated a diffuse SAH predominantly in the Sylvian and suprasellar cisterns. Patients were admitted to the neuro intensive care unit and underwent diagnostic angiograms to identify possible aneurysms. Magnetic resonance imaging and angiograms for both patients were negative. Patients were managed with best medical therapy and followed up in the outpatient setting. Unilateral CNIII palsy in the setting of NASAH was identified in both patients. Diagnostic angiograms were negative for aneurysms; therefore, SAH were determined to be spontaneous. We propose that unilateral CNIII palsy is a possible sign of NASAH.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
