Protective continuous ventilation strategy during cardiopulmonary bypass in children undergoing surgery for congenital heart disease: a prospective study.
Massimo A Padalino, Luca Vedovelli, Manuela Simonato, Andrea Bandini, Greta Paganini, Laura Mezzalira, Nicola Faganello, Cristiana Carollo, Dario Gregori, Vladimiro Vida, Paola Cogo
{"title":"Protective continuous ventilation strategy during cardiopulmonary bypass in children undergoing surgery for congenital heart disease: a prospective study.","authors":"Massimo A Padalino, Luca Vedovelli, Manuela Simonato, Andrea Bandini, Greta Paganini, Laura Mezzalira, Nicola Faganello, Cristiana Carollo, Dario Gregori, Vladimiro Vida, Paola Cogo","doi":"10.1093/icvts/ivac084","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to evaluate if a 'protective' (low-tidal/low-frequency) ventilation strategy can shorten the postoperative ventilation time and minimize acute lung injury in children with congenital heart disease (CHD) undergoing repair with cardiopulmonary bypass (CPB).</p><p><strong>Methods: </strong>This is a single-centre prospective, interventional study, including children with CHD under the age of 5 years, undergoing open-heart surgery with a CPB >60 min, in hypothermia, haemodynamically stable, and without evident genetic abnormalities. Assist-control ventilation (tidal volume of 4 ml/kg, 10 breaths/min, positive end-expiratory pressure 5 cmH2O and FiO2 0.21) was applied in a cohort of patients during CPB. We compared clinical outcomes and in fully ventilated versus non-ventilated (control) patients. Propensity score was used to weigh ventilated and control groups to correct for the effect of other confounding clinical variables. Clinical and ventilation parameters and lung inflammatory biomarkers in tracheal aspirates were measured. The primary outcome was the postoperative intubation time of more or less than 48 h.</p><p><strong>Results: </strong>We included 140 children (53 ventilated, 87 non-ventilated) with different CHD. There were no deaths or adverse events in ventilated patients. Using a weighted generalized linear model, we found no sufficient evidence for an effect of intraoperative ventilation on postoperative intubation time [estimate 0.13 (95% confidence interval, -0.08; 0.35), P = 0.22].</p><p><strong>Conclusions: </strong>Continuous low-tidal/low-frequency mechanical ventilation during CPB is safe and harmless. However, no significant advantages were found when compared to non-ventilated patients in terms of postoperative ventilation time.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9297524/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac084","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
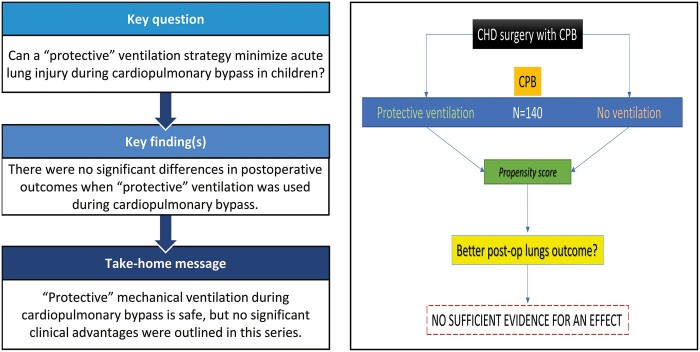
Objectives: The aim of this study was to evaluate if a 'protective' (low-tidal/low-frequency) ventilation strategy can shorten the postoperative ventilation time and minimize acute lung injury in children with congenital heart disease (CHD) undergoing repair with cardiopulmonary bypass (CPB).
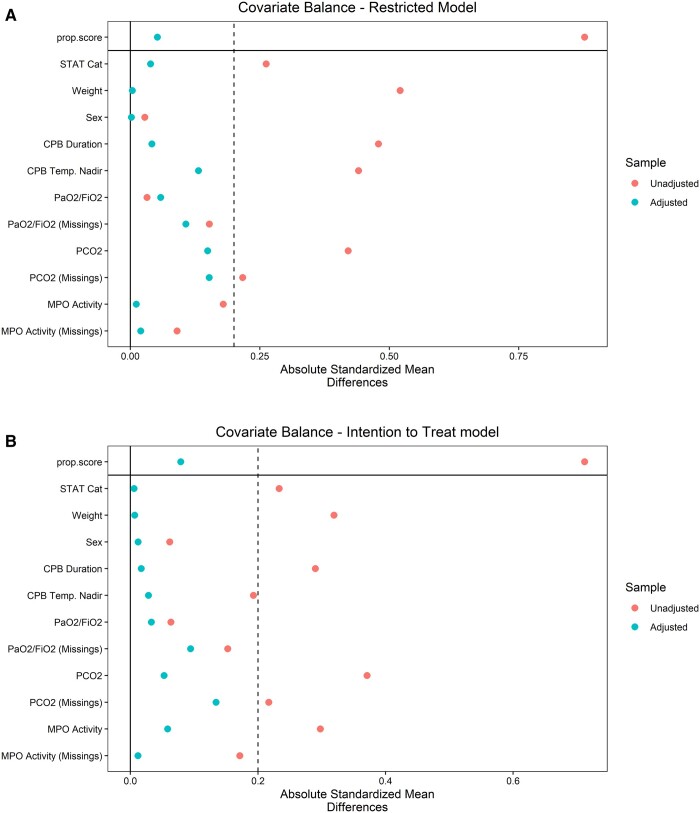
Methods: This is a single-centre prospective, interventional study, including children with CHD under the age of 5 years, undergoing open-heart surgery with a CPB >60 min, in hypothermia, haemodynamically stable, and without evident genetic abnormalities. Assist-control ventilation (tidal volume of 4 ml/kg, 10 breaths/min, positive end-expiratory pressure 5 cmH2O and FiO2 0.21) was applied in a cohort of patients during CPB. We compared clinical outcomes and in fully ventilated versus non-ventilated (control) patients. Propensity score was used to weigh ventilated and control groups to correct for the effect of other confounding clinical variables. Clinical and ventilation parameters and lung inflammatory biomarkers in tracheal aspirates were measured. The primary outcome was the postoperative intubation time of more or less than 48 h.
Results: We included 140 children (53 ventilated, 87 non-ventilated) with different CHD. There were no deaths or adverse events in ventilated patients. Using a weighted generalized linear model, we found no sufficient evidence for an effect of intraoperative ventilation on postoperative intubation time [estimate 0.13 (95% confidence interval, -0.08; 0.35), P = 0.22].
Conclusions: Continuous low-tidal/low-frequency mechanical ventilation during CPB is safe and harmless. However, no significant advantages were found when compared to non-ventilated patients in terms of postoperative ventilation time.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
