Alexandra Nguyen, Catherine Tran, Aldin Malkoc, Vivian Davis, Michael M Neeki
{"title":"Development of Early Abdominal Compartment Syndrome Leading to Emergent Decompressive Laparotomy in Full-Thickness Burn Injury.","authors":"Alexandra Nguyen, Catherine Tran, Aldin Malkoc, Vivian Davis, Michael M Neeki","doi":"10.14740/jmc3970","DOIUrl":null,"url":null,"abstract":"<p><p>Burn injuries carry an increased risk of intra-abdominal hypertension and are an independent risk factor for abdominal compartment syndrome (ACS). ACS is most commonly due to large volume resuscitation. The added concern of ACS can complicate resuscitative efforts. Early monitoring for ACS (intra-abdominal pressure > 20 mm Hg with associated new-onset organ dysfunction) and performing prudent decompressive laparotomies are important factors to keep in mind when treating large surface area burn patients. This case report describes the hospitalization of a 60-year-old male who presented with 45% full-thickness (FT) total body surface area (TBSA) and inhalation injury. On arrival to the emergency department (ED), he had received a total of 6 L of intravenous lactate Ringers, and vasopressors were initiated due to hypotension. During the tertiary examination it was noted that there was increased difficulty ventilating the patient, and his abdomen was becoming increasingly distended and tense. His intra-abdominal pressure was measured in the ED and found to be elevated at 32 mm Hg. The findings were suggestive of ACS and a decompressive laparotomy was performed in the ED. Upon entering the abdominal cavity, the abdominal contents extruded through the incision and diffuse venous congestion and gastric distention were noted. Items commonly found in operating rooms (Top-Draper<sup>®</sup> warmer drape, Kerlix rolls, Jackson-Pratt suction drains, and 3M<sup>®</sup> Ioban sterile antimicrobial incise drape) were utilized to maintain an open abdomen where abdominal contents could easily be observed and to prevent delay in performing a decompressive laparotomy. Here we describe a patient with 45% FT TBSA and inhalation injuries requiring an emergent decompressive laparotomy for ACS after only 6 L of lactate Ringers were administered. This highlights the importance of early monitoring for ACS and the ease of performing a decompressive laparotomy with commonly found items in the ED and operating rooms.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"13 9","pages":"438-442"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bd/2d/jmc-13-438.PMC9534200.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc3970","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/28 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
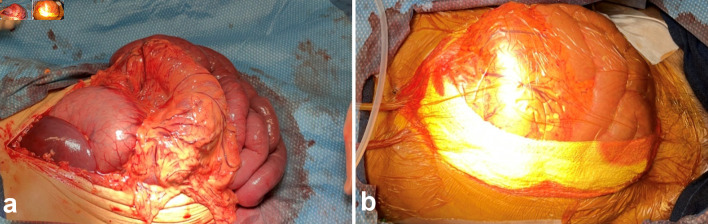
Burn injuries carry an increased risk of intra-abdominal hypertension and are an independent risk factor for abdominal compartment syndrome (ACS). ACS is most commonly due to large volume resuscitation. The added concern of ACS can complicate resuscitative efforts. Early monitoring for ACS (intra-abdominal pressure > 20 mm Hg with associated new-onset organ dysfunction) and performing prudent decompressive laparotomies are important factors to keep in mind when treating large surface area burn patients. This case report describes the hospitalization of a 60-year-old male who presented with 45% full-thickness (FT) total body surface area (TBSA) and inhalation injury. On arrival to the emergency department (ED), he had received a total of 6 L of intravenous lactate Ringers, and vasopressors were initiated due to hypotension. During the tertiary examination it was noted that there was increased difficulty ventilating the patient, and his abdomen was becoming increasingly distended and tense. His intra-abdominal pressure was measured in the ED and found to be elevated at 32 mm Hg. The findings were suggestive of ACS and a decompressive laparotomy was performed in the ED. Upon entering the abdominal cavity, the abdominal contents extruded through the incision and diffuse venous congestion and gastric distention were noted. Items commonly found in operating rooms (Top-Draper® warmer drape, Kerlix rolls, Jackson-Pratt suction drains, and 3M® Ioban sterile antimicrobial incise drape) were utilized to maintain an open abdomen where abdominal contents could easily be observed and to prevent delay in performing a decompressive laparotomy. Here we describe a patient with 45% FT TBSA and inhalation injuries requiring an emergent decompressive laparotomy for ACS after only 6 L of lactate Ringers were administered. This highlights the importance of early monitoring for ACS and the ease of performing a decompressive laparotomy with commonly found items in the ED and operating rooms.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
