Monique Freire, Viviane Carvalho, Renata Spener, Christiane Rodrigues da Silva, João Ricardo da Silva Neto, Luiz Carlos Ferreira, Paulo Afonso Nogueira
{"title":"Hemophagocytic Syndrome in a Patient with HIV and Histoplasmosis: A not so Rare Correlation.","authors":"Monique Freire, Viviane Carvalho, Renata Spener, Christiane Rodrigues da Silva, João Ricardo da Silva Neto, Luiz Carlos Ferreira, Paulo Afonso Nogueira","doi":"10.1177/2632010X221118059","DOIUrl":null,"url":null,"abstract":"<p><p>Hemophagocytic lymphohistiocytosis (HLH) is a disorder that occurs due to unsuitable monocyte activation in a variety of infections. In human immunodeficiency virus (HIV) infections, patients with advanced immunossupression associated with opportunistic infections are at increased risk of developing HLH. We describe a clinical case of a 33-year-old male student diagnosed with HIV who was hospitalized for investigation of asthenia and dyspnea, accompanied by adynamia, decreased motor force in the left leg, dysphagia, and dysfluency. His general condition was regular, he was pale, feverish, and had normal cardiac and pulmonary auscultation. Physical examination revealed ulcerated lesions in the perianal region and hepatosplenomegaly without palpable lymph node enlargement. Laboratory parameters showed pancytopenia, a slight increase in liver function accompanied by high lactate dehydrogenase, and hiperferritinemia. The initial diagnosis was disseminated histoplasmosis, thus amphotericin B deoxycholate was empirically prescribed while waiting on myeloculture and blood cultures for fungi and mycobacteria. Other clinical procedures were blood transfusion, resumption of antiretroviral therapy (ART) and secondary prophylaxis. Myeloculture blood cultures of fungi and mycobacteria were negative. Patient evolved well in relation to the initial complaints and showed partial clinical and laboratory improvement. However, 23 days after hospitalization, he developed a febrile episode accompanied by chills and a convulsive crisis. The patient was transferred to the intensive unit care and developed septic shock and respiratory failure. He died 25 days after the onset of the condition. After the postmortem examination, histopathology revealed countless rounded fungal structures compatible with <i>Histoplasma</i> sp., which were observed in the peripancreatic lymph node, liver, and spleen, in addition to hemophagocytosis in the splenic parenchyma. We thus conclude that when the patient met criteria for HLH, such as fever, hepatosplenomegaly, hiperferritinemia, and pancytopenia, the evolution was fast due to the aggressive and rapidly fatal nature of HLH, despite anti-fungal and corticoid treatment. Therefore, this case report reinforces the need to consider hemophagocytic syndrome in patients with HIV and disseminated histoplasmosis, especially where histoplasmosis is highly endemic, in order for the treatment be started early when there is high clinical suspicion.</p>","PeriodicalId":53204,"journal":{"name":"Clinical Pathology","volume":" ","pages":"2632010X221118059"},"PeriodicalIF":1.9000,"publicationDate":"2022-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8f/65/10.1177_2632010X221118059.PMC9425888.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2632010X221118059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
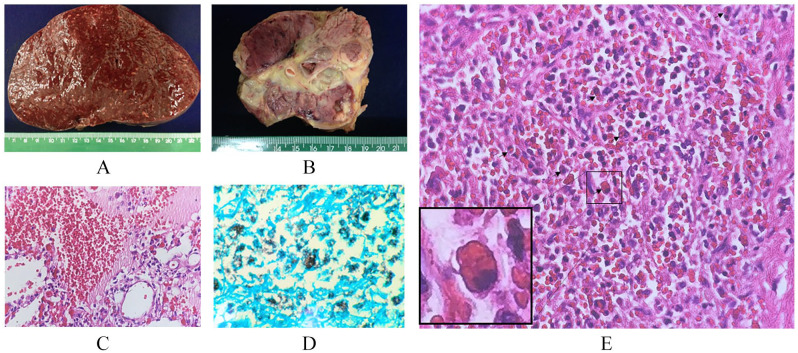
Hemophagocytic lymphohistiocytosis (HLH) is a disorder that occurs due to unsuitable monocyte activation in a variety of infections. In human immunodeficiency virus (HIV) infections, patients with advanced immunossupression associated with opportunistic infections are at increased risk of developing HLH. We describe a clinical case of a 33-year-old male student diagnosed with HIV who was hospitalized for investigation of asthenia and dyspnea, accompanied by adynamia, decreased motor force in the left leg, dysphagia, and dysfluency. His general condition was regular, he was pale, feverish, and had normal cardiac and pulmonary auscultation. Physical examination revealed ulcerated lesions in the perianal region and hepatosplenomegaly without palpable lymph node enlargement. Laboratory parameters showed pancytopenia, a slight increase in liver function accompanied by high lactate dehydrogenase, and hiperferritinemia. The initial diagnosis was disseminated histoplasmosis, thus amphotericin B deoxycholate was empirically prescribed while waiting on myeloculture and blood cultures for fungi and mycobacteria. Other clinical procedures were blood transfusion, resumption of antiretroviral therapy (ART) and secondary prophylaxis. Myeloculture blood cultures of fungi and mycobacteria were negative. Patient evolved well in relation to the initial complaints and showed partial clinical and laboratory improvement. However, 23 days after hospitalization, he developed a febrile episode accompanied by chills and a convulsive crisis. The patient was transferred to the intensive unit care and developed septic shock and respiratory failure. He died 25 days after the onset of the condition. After the postmortem examination, histopathology revealed countless rounded fungal structures compatible with Histoplasma sp., which were observed in the peripancreatic lymph node, liver, and spleen, in addition to hemophagocytosis in the splenic parenchyma. We thus conclude that when the patient met criteria for HLH, such as fever, hepatosplenomegaly, hiperferritinemia, and pancytopenia, the evolution was fast due to the aggressive and rapidly fatal nature of HLH, despite anti-fungal and corticoid treatment. Therefore, this case report reinforces the need to consider hemophagocytic syndrome in patients with HIV and disseminated histoplasmosis, especially where histoplasmosis is highly endemic, in order for the treatment be started early when there is high clinical suspicion.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
