Successful Treatment of Intracranial Methotrexate-associated Lymphoproliferative Disorder without Epstein-Barr Virus Infection Using Rituximab, Methotrexate, Procarbazine, and Vincristine: A Case Report.
{"title":"Successful Treatment of Intracranial Methotrexate-associated Lymphoproliferative Disorder without Epstein-Barr Virus Infection Using Rituximab, Methotrexate, Procarbazine, and Vincristine: A Case Report.","authors":"Makoto Mizushima, Yukitomo Ishi, Hiroshi Ikeda, Ikuma Echizenya, Takuya Otsuka, Tomoko Mitsuhashi, Shigeru Yamaguchi, Miki Fujimura","doi":"10.2176/jns-nmc.2022-0091","DOIUrl":null,"url":null,"abstract":"<p><p>Methotrexate-associated lymphoproliferative disorder (MTX-LPD) occurs in patients with rheumatoid arthritis (RA) treated with methotrexate (MTX). MTX-LPD is typically associated with Epstein-Barr virus (EBV) infection and regresses with MTX discontinuation. On the other hand, EBV-negative MTX-LPDs are less common and are more likely to show partial or no regression after MTX discontinuation. There were no standard chemotherapeutic options for refractory MTX-LPD. We present a case of EBV-negative MTX-LPD in the central nervous system (CNS) that was successfully treated with rituximab, methotrexate, procarbazine, and vincristine (R-MPV), followed by reduced-dose whole-brain radiotherapy (rdWBRT), following the same treatment protocol as primary CNS lymphoma. A 59-year-old woman with RA treated with MTX presented with gradually developing staggered gait, memory deficit, and disorientation. Multiple lesions with heterogeneous contrast enhancement were discovered using brain magnetic resonance imaging. The patient was suspected of having MTX-LPD, but discontinuing MTX did not result in regression of the brain lesions. She underwent a biopsy from the left parietal lesion. The tissue was pathologically diagnosed as diffuse large B-cell lymphoma. Furthermore, pathological examination through EBV-encoded ribonucleic acid <i>in situ</i> hybridization demonstrated a lack of EBV infection. She was ultimately diagnosed with EBV-negative CNS MTX-LPD. We applied chemotherapy with R-MPV and rdWBRT. The patient achieved a complete response. In the case of CNS MTX-LPD without EBV infection, chemotherapy with R-MPV followed by rdWBRT may be considered.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":" ","pages":"237-242"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/21/57/2188-4226-9-0237.PMC9398467.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
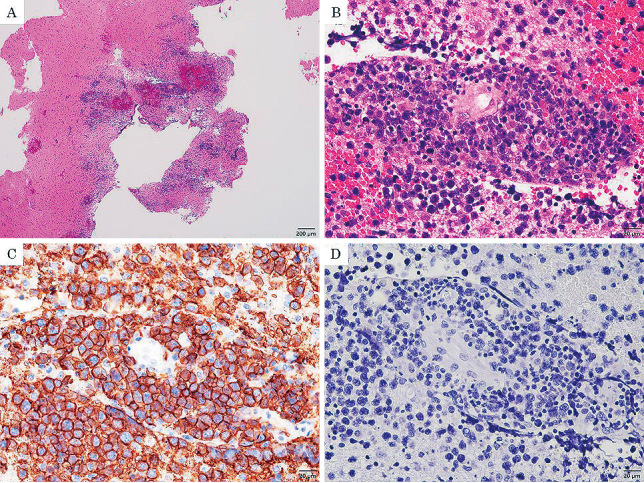
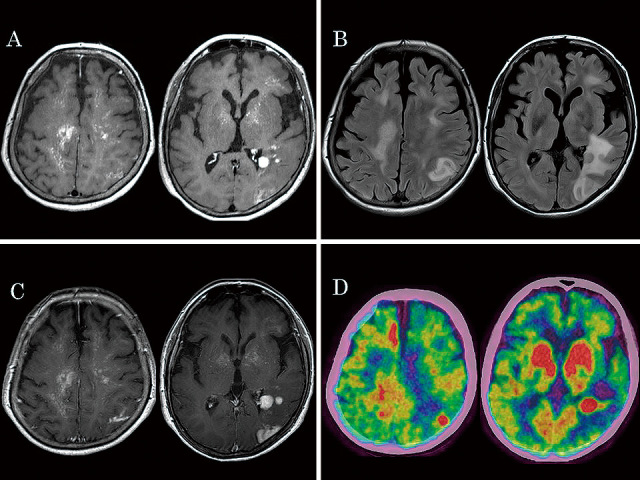
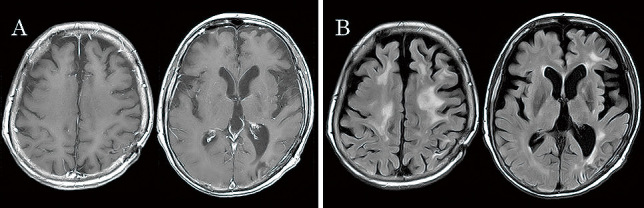
Methotrexate-associated lymphoproliferative disorder (MTX-LPD) occurs in patients with rheumatoid arthritis (RA) treated with methotrexate (MTX). MTX-LPD is typically associated with Epstein-Barr virus (EBV) infection and regresses with MTX discontinuation. On the other hand, EBV-negative MTX-LPDs are less common and are more likely to show partial or no regression after MTX discontinuation. There were no standard chemotherapeutic options for refractory MTX-LPD. We present a case of EBV-negative MTX-LPD in the central nervous system (CNS) that was successfully treated with rituximab, methotrexate, procarbazine, and vincristine (R-MPV), followed by reduced-dose whole-brain radiotherapy (rdWBRT), following the same treatment protocol as primary CNS lymphoma. A 59-year-old woman with RA treated with MTX presented with gradually developing staggered gait, memory deficit, and disorientation. Multiple lesions with heterogeneous contrast enhancement were discovered using brain magnetic resonance imaging. The patient was suspected of having MTX-LPD, but discontinuing MTX did not result in regression of the brain lesions. She underwent a biopsy from the left parietal lesion. The tissue was pathologically diagnosed as diffuse large B-cell lymphoma. Furthermore, pathological examination through EBV-encoded ribonucleic acid in situ hybridization demonstrated a lack of EBV infection. She was ultimately diagnosed with EBV-negative CNS MTX-LPD. We applied chemotherapy with R-MPV and rdWBRT. The patient achieved a complete response. In the case of CNS MTX-LPD without EBV infection, chemotherapy with R-MPV followed by rdWBRT may be considered.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
