{"title":"A contemporary snippet on clinical presentation and management of toxic epidermal necrolysis.","authors":"Piyu Parth Naik","doi":"10.1177/20595131221122381","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Toxic epidermal necrolysis (TEN) is one of the most severe cutaneous adverse reactions with a mortality rate of 30%. Due to a lack of consensus regarding the treatment and management of TEN, therapy is individualized on a case-to-case basis.</p><p><strong>Purpose: </strong>The scientific literature about Stevens-Johnson Syndrome (SJS) and TEN is summarized and assessed to aid and assist in determining the optimal course of treatment.</p><p><strong>Methods: </strong>PubMed and Google Scholar, among others, were searched with the keywords: \"Toxic Epidermal Necrolysis\", \"corticosteroids\", \"cyclosporine\", \"etanercept\", \"intravenous immunoglobulin\", \"Stevens-Johnson syndrome\" and filtered by year. The research articles generated by the search, and their references, were reviewed.</p><p><strong>Results: </strong>TEN is a severe dermatological condition that is mainly caused by medicines. World-wide guidelines differ in care plans. As there is no consensus on the management of TEN, this article aims to summarize the efficacy and feasibility of the management aspect of TEN from previous studies. Supportive care is highly accepted, along with early discontinuation of all medicines (hydration & electrolytes). Corticosteroids and cyclosporine have been used in therapy. Intravenous immunoglobulin (IVIG) is currently being administered; however, their efficacy by themselves and in combination remains uncertain.</p><p><strong>Conclusion: </strong>Current evidence predominantly from retrospective studies suggests no individual treatment has sufficient efficacy and a multi-faceted regimen stands to be favored. Therapeutic regimens from corticosteroids to IVIG are under constant evaluation. The life-threatening nature of TEN warrants further confirmation with more extensive, robust randomized, controlled trials.</p><p><strong>Lay summary: </strong>Toxic epidermal necrolysis (TEN) is a serious skin reaction with a 30% chance of mortality. Commonly TEN is caused by medicines and results in a burn like appearance and sensation in patients. Usually administered medicine is cleared effectively by the human body but when the clearance of few metabolites from medicine is disrupted due to few genes, it leads to an ominous response by the body. This response involves several intermediate chemicals that primarily attack skin cells. Treatment guidelines differ globally. Supportive care is highly accepted, along with early discontinuation of all medicine. Currently, a multi-faceted treatment regimen is favored. Treatments like corticosteroids to immunoglobulins are under constant evaluation. Identification of the perfect combination of treatment needs confirmation from robust randomized controlled trials.</p>","PeriodicalId":21495,"journal":{"name":"Scars, burns & healing","volume":" ","pages":"20595131221122381"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c1/35/10.1177_20595131221122381.PMC9476246.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scars, burns & healing","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20595131221122381","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: Toxic epidermal necrolysis (TEN) is one of the most severe cutaneous adverse reactions with a mortality rate of 30%. Due to a lack of consensus regarding the treatment and management of TEN, therapy is individualized on a case-to-case basis.
Purpose: The scientific literature about Stevens-Johnson Syndrome (SJS) and TEN is summarized and assessed to aid and assist in determining the optimal course of treatment.
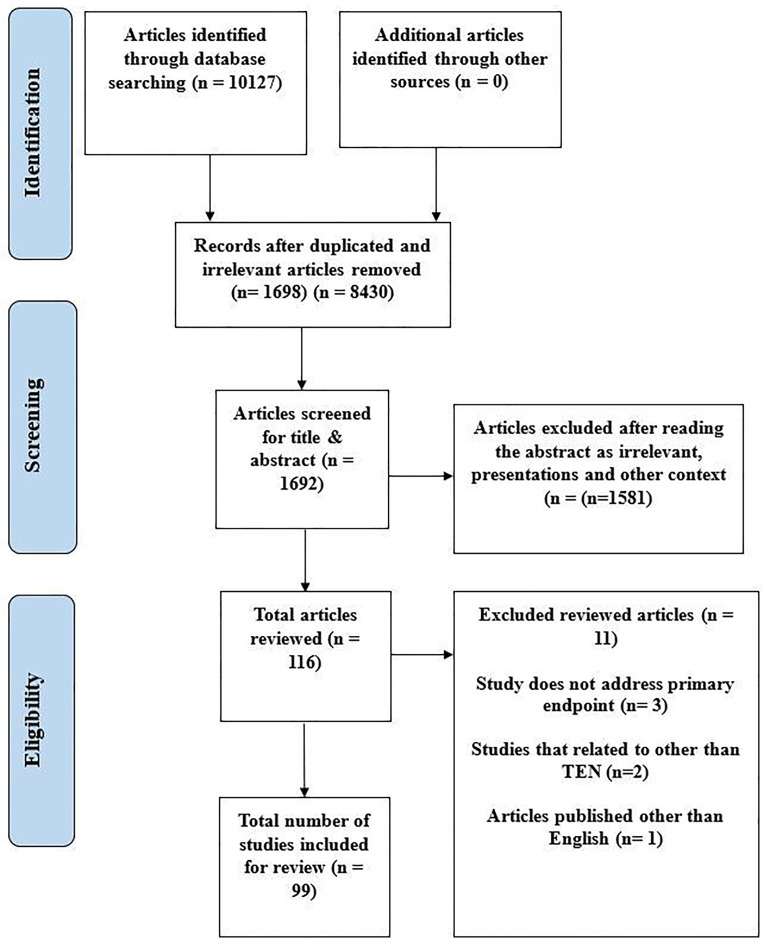
Methods: PubMed and Google Scholar, among others, were searched with the keywords: "Toxic Epidermal Necrolysis", "corticosteroids", "cyclosporine", "etanercept", "intravenous immunoglobulin", "Stevens-Johnson syndrome" and filtered by year. The research articles generated by the search, and their references, were reviewed.
Results: TEN is a severe dermatological condition that is mainly caused by medicines. World-wide guidelines differ in care plans. As there is no consensus on the management of TEN, this article aims to summarize the efficacy and feasibility of the management aspect of TEN from previous studies. Supportive care is highly accepted, along with early discontinuation of all medicines (hydration & electrolytes). Corticosteroids and cyclosporine have been used in therapy. Intravenous immunoglobulin (IVIG) is currently being administered; however, their efficacy by themselves and in combination remains uncertain.
Conclusion: Current evidence predominantly from retrospective studies suggests no individual treatment has sufficient efficacy and a multi-faceted regimen stands to be favored. Therapeutic regimens from corticosteroids to IVIG are under constant evaluation. The life-threatening nature of TEN warrants further confirmation with more extensive, robust randomized, controlled trials.
Lay summary: Toxic epidermal necrolysis (TEN) is a serious skin reaction with a 30% chance of mortality. Commonly TEN is caused by medicines and results in a burn like appearance and sensation in patients. Usually administered medicine is cleared effectively by the human body but when the clearance of few metabolites from medicine is disrupted due to few genes, it leads to an ominous response by the body. This response involves several intermediate chemicals that primarily attack skin cells. Treatment guidelines differ globally. Supportive care is highly accepted, along with early discontinuation of all medicine. Currently, a multi-faceted treatment regimen is favored. Treatments like corticosteroids to immunoglobulins are under constant evaluation. Identification of the perfect combination of treatment needs confirmation from robust randomized controlled trials.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
