Chlamydia pneumoniae is Prevalent in Symptomatic Coronary Atherosclerotic Plaque Samples Obtained From Directional Coronary Atherectomy, but its Quantity is Not Associated With Plaque Instability: An Immunohistochemical and Molecular Study.
{"title":"<i>Chlamydia pneumoniae</i> is Prevalent in Symptomatic Coronary Atherosclerotic Plaque Samples Obtained From Directional Coronary Atherectomy, but its Quantity is Not Associated With Plaque Instability: An Immunohistochemical and Molecular Study.","authors":"Tomoyuki Otani, Kensaku Nishihira, Yoshinao Azuma, Atsushi Yamashita, Yoshisato Shibata, Yujiro Asada, Kinta Hatakeyama","doi":"10.1177/2632010X221125179","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To clarify whether there is any association between the extent of <i>Chlamydia pneumoniae (C. pneumoniae</i>) infection and plaque instability or post-directional coronary atherectomy (DCA) restenosis, we determined the frequency of <i>C. pneumoniae</i> infection and its localization in symptomatic coronary atherosclerotic plaques using specimens obtained from DCA.</p><p><strong>Methods and results: </strong>Immunohistochemistry (IHC) and real-time polymerase chain reaction (RT-PCR) revealed the existence of <i>C. pneumoniae</i> in all 50 specimens of coronary atherosclerotic plaques obtained by DCA. <i>C. pneumoniae</i>-positive cell ratio determined with IHC or copy numbers of <i>C. pneumoniae</i> DNA detected by RT-PCR did not differ significantly between patients with stable angina pectoris and those with acute coronary syndrome (IHC: 16.4 ± 7.6% vs 18.0 ± 7.1%, <i>P</i> = .42; RT-PCR: no. of cases with high copy numbers 12/25 vs 10/25, <i>P</i> = .78), or between patients with subsequent post-DCA restenosis and those without (IHC: 17.1 ± 8.0% vs 18.0 ± 7.4%, <i>P</i> = .74; RT-PCR: 5/12 vs 10/21, <i>P</i> = 1.00).</p><p><strong>Conclusions: </strong><i>C. pneumoniae</i> was highly prevalent in coronary atherosclerotic plaques of patients who underwent DCA. However, the extent of <i>C. pneumoniae</i> infection in coronary atherosclerotic plaques was not associated with plaque instability or post-DCA restenosis.</p>","PeriodicalId":53204,"journal":{"name":"Clinical Pathology","volume":" ","pages":"2632010X221125179"},"PeriodicalIF":1.9000,"publicationDate":"2022-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2a/61/10.1177_2632010X221125179.PMC9513565.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2632010X221125179","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To clarify whether there is any association between the extent of Chlamydia pneumoniae (C. pneumoniae) infection and plaque instability or post-directional coronary atherectomy (DCA) restenosis, we determined the frequency of C. pneumoniae infection and its localization in symptomatic coronary atherosclerotic plaques using specimens obtained from DCA.
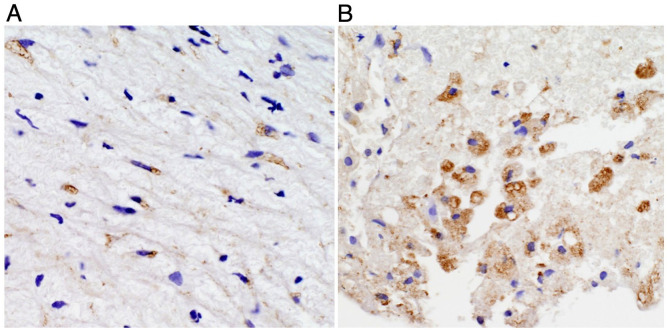
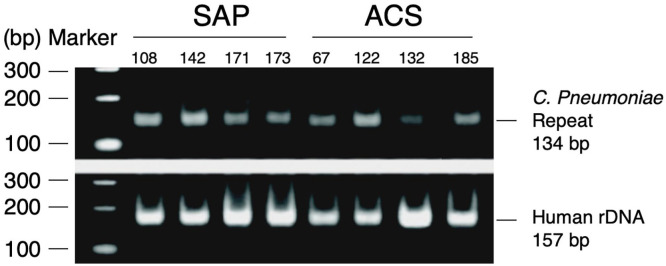
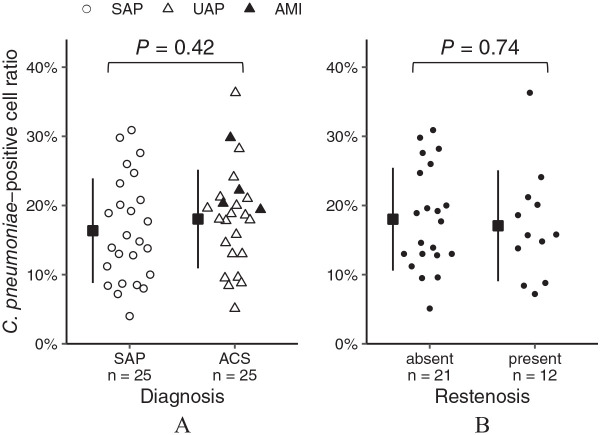
Methods and results: Immunohistochemistry (IHC) and real-time polymerase chain reaction (RT-PCR) revealed the existence of C. pneumoniae in all 50 specimens of coronary atherosclerotic plaques obtained by DCA. C. pneumoniae-positive cell ratio determined with IHC or copy numbers of C. pneumoniae DNA detected by RT-PCR did not differ significantly between patients with stable angina pectoris and those with acute coronary syndrome (IHC: 16.4 ± 7.6% vs 18.0 ± 7.1%, P = .42; RT-PCR: no. of cases with high copy numbers 12/25 vs 10/25, P = .78), or between patients with subsequent post-DCA restenosis and those without (IHC: 17.1 ± 8.0% vs 18.0 ± 7.4%, P = .74; RT-PCR: 5/12 vs 10/21, P = 1.00).
Conclusions: C. pneumoniae was highly prevalent in coronary atherosclerotic plaques of patients who underwent DCA. However, the extent of C. pneumoniae infection in coronary atherosclerotic plaques was not associated with plaque instability or post-DCA restenosis.
目的:为了阐明肺炎衣原体(C. pneumoniae)感染程度与斑块不稳定性或定向冠状动脉粥样硬化切除术(DCA)后再狭窄之间是否存在关联,我们利用从DCA获得的标本确定了肺炎衣原体感染的频率及其在症状性冠状动脉粥样硬化斑块中的定位。方法与结果:免疫组化(IHC)和实时聚合酶链反应(RT-PCR)显示50例冠状动脉粥样硬化斑块标本均存在肺炎原体。稳定型心绞痛患者与急性冠状动脉综合征患者间采用免疫组化检测肺炎原体阳性细胞比例或RT-PCR检测肺炎原体DNA拷贝数无显著差异(免疫组化:16.4±7.6% vs 18.0±7.1%,P = 0.42;rt - pcr:没有。高拷贝数患者(12/25 vs 10/25, P = 0.78),或dca后再狭窄患者与无dca后再狭窄患者(IHC: 17.1±8.0% vs 18.0±7.4%,P = 0.74;RT-PCR: 5/12 vs 10/21, P = 1.00)。结论:肺炎原体在行DCA患者的冠状动脉粥样硬化斑块中高度流行。然而,冠状动脉粥样硬化斑块中肺炎支原体感染的程度与斑块不稳定或dca后再狭窄无关。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
