Mika L Nonoyama, Vinay Kukreti, Efrosini Papaconstantinou, Natascha Kozlowski, Sarah Tsimelkas
{"title":"Outcomes and follow-up for children intubated in an adult-based community hospital system: A retrospective chart review.","authors":"Mika L Nonoyama, Vinay Kukreti, Efrosini Papaconstantinou, Natascha Kozlowski, Sarah Tsimelkas","doi":"10.29390/cjrt-2022-015","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Emergency intubation is a high-risk procedure in children. Studies describing intubation practices in locations other than pediatric centres are scarce and varied. This study described pediatric intubations in adult-based community emergency departments (EDs) and determined what factors were associated with intubated-related adverse events (AEs) and described outcomes of children transferred to a quaternary care pediatric institution.</p><p><strong>Methods: </strong>This is a retrospective review of data collected between January 2006 and March 2017 at Lakeridge Health and Hospital for Sick Children (SickKids). Patients were <18 years and intubated in Lakeridge Health EDs; those intubated prior to ED arrival were excluded. Primary outcomes were intubation first-pass success (FPS) and AEs secondary to intubation.</p><p><strong>Results: </strong>Patients (<i>n</i> = 121) were analyzed, and median (interquartile range (IQR)) age was 3.7 (0.4-14.3) years. There were 76 (62.8%) FPS, with no difference between pediatricians (<i>n</i> = 25, 23%) or anaesthetists (<i>n =</i> 12, 11%), versus all other providers (paramedic <i>n =</i> 13 (12%), ED physician <i>n =</i> 37 (34%), respiratory therapist <i>n =</i> 20 (18%), transfer team <i>n =</i> 2 (2%)). The proportion of AEs was 24 (19.8%, <i>n =</i> 21 minor, <i>n =</i> 3 major), with no significant difference between pediatricians or anaesthetists versus all other providers. Data from 68 children transferred to SickKids were available, with the majority extubated within a short median (IQR) time of admission, 1.2 (0.29-3.8) days.</p><p><strong>Conclusions: </strong>Pediatric intubations were rare in a Canadian adult-based community hospital system. Most intubations demonstrated FPS with relatively few AEs and no significant differences between health provider type. Future investigations should utilize multi-centred data to inform strategies suited for organizations' unique practice cultures, including training programs.</p>","PeriodicalId":39373,"journal":{"name":"Canadian Journal of Respiratory Therapy","volume":" ","pages":"69-76"},"PeriodicalIF":1.1000,"publicationDate":"2022-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/a0/cjrt-2022-015.PMC9187052.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Respiratory Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.29390/cjrt-2022-015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"0","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Emergency intubation is a high-risk procedure in children. Studies describing intubation practices in locations other than pediatric centres are scarce and varied. This study described pediatric intubations in adult-based community emergency departments (EDs) and determined what factors were associated with intubated-related adverse events (AEs) and described outcomes of children transferred to a quaternary care pediatric institution.
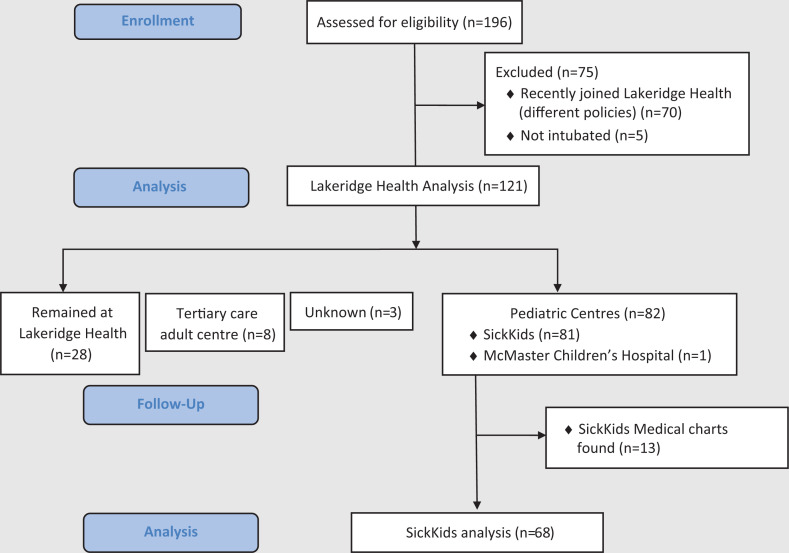
Methods: This is a retrospective review of data collected between January 2006 and March 2017 at Lakeridge Health and Hospital for Sick Children (SickKids). Patients were <18 years and intubated in Lakeridge Health EDs; those intubated prior to ED arrival were excluded. Primary outcomes were intubation first-pass success (FPS) and AEs secondary to intubation.
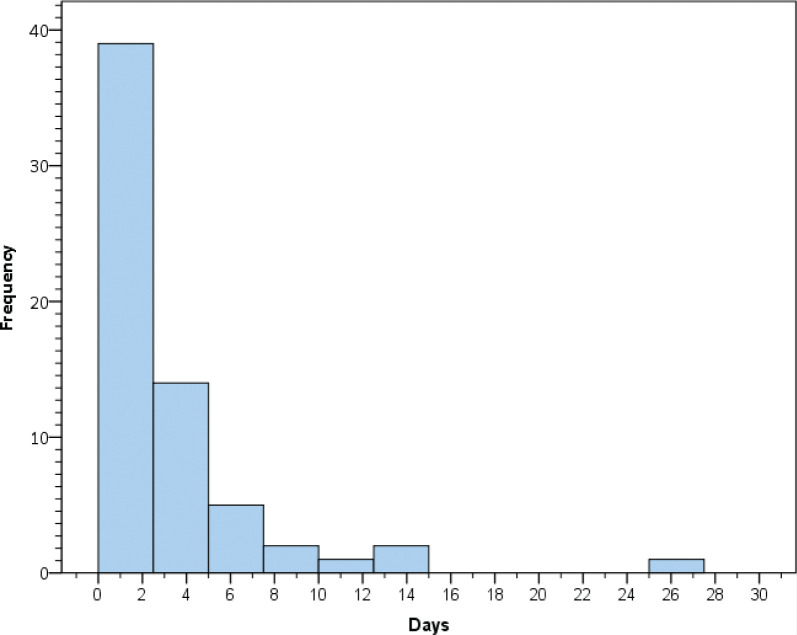
Results: Patients (n = 121) were analyzed, and median (interquartile range (IQR)) age was 3.7 (0.4-14.3) years. There were 76 (62.8%) FPS, with no difference between pediatricians (n = 25, 23%) or anaesthetists (n = 12, 11%), versus all other providers (paramedic n = 13 (12%), ED physician n = 37 (34%), respiratory therapist n = 20 (18%), transfer team n = 2 (2%)). The proportion of AEs was 24 (19.8%, n = 21 minor, n = 3 major), with no significant difference between pediatricians or anaesthetists versus all other providers. Data from 68 children transferred to SickKids were available, with the majority extubated within a short median (IQR) time of admission, 1.2 (0.29-3.8) days.
Conclusions: Pediatric intubations were rare in a Canadian adult-based community hospital system. Most intubations demonstrated FPS with relatively few AEs and no significant differences between health provider type. Future investigations should utilize multi-centred data to inform strategies suited for organizations' unique practice cultures, including training programs.
期刊介绍:
The CJRT is published four times a year and represents the interests of respiratory therapists nationally and internationally. The CJRT has been redesigned to act as an educational dissemination tool. The CJRT encourages submission of original articles, papers, commentaries, case studies, literature reviews and directed reading papers. Submissions can be sent to Rita Hansen.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
