K Anderson, E Pietersen, K Dheda, Y F van der Heijden
{"title":"Comparison of treatment outcome definitions in drug-resistant tuberculosis patients with high incidence of acquired second-line drug resistance.","authors":"K Anderson, E Pietersen, K Dheda, Y F van der Heijden","doi":"10.7196/AJTCCM.2022.v28i2.177","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Simplified drug-resistant tuberculosis (DR-TB) treatment outcome definitions, mostly centred around receipt of treatment and sputum culture status at 6 months after treatment initiation, have been proposed, but have not been widely evaluated in resource-limited settings.</p><p><strong>Objectives: </strong>To compare DR-TB treatment outcomes, as defined by the World Health Organization (WHO) at the time of treatment, with simplified definitions.</p><p><strong>Methods: </strong>We performed retrospective folder reviews of a cohort of 246 South African DR-TB patients, most of whom developed second-line drug resistance. Sequential treatment outcomes were assigned retrospectively using both simplified Tuberculosis Network European Trials Group (TBNET)-based and 2013 WHO-based definitions.</p><p><strong>Results: </strong>Of 246 patients, 40% were HIV-positive, and 88% developed second-line drug resistance. Patients were observed for a median of 38 (interquartile range 24 - 63) months from DR-TB treatment initiation. Using WHO-based definitions, 93% of patients had >1 sequential outcome, whereas with simplified definitions, 25% of patients had >1 outcome. Fewer outcomes of cure (3% v. 9%) and more outcomes of treatment failure (42% v. 22%) were assigned using simplified definitions.</p><p><strong>Conclusion: </strong>Simplified outcome definitions applied to real-world patients with long, often complex treatment histories resulted in underestimating cures and overestimating treatment failures compared with WHO-based definitions. Simplified definitions may identify more individuals at higher risk for treatment failure than WHO-based definitions, but without consistent programmatic follow-up it may be difficult to distinguish cure, failure and loss to follow-up.</p>","PeriodicalId":52847,"journal":{"name":"African Journal of Thoracic and Critical Care Medicine","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2022-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e0/5d/AJTCCM-28-2-177.PMC9379990.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Thoracic and Critical Care Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/AJTCCM.2022.v28i2.177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Simplified drug-resistant tuberculosis (DR-TB) treatment outcome definitions, mostly centred around receipt of treatment and sputum culture status at 6 months after treatment initiation, have been proposed, but have not been widely evaluated in resource-limited settings.
Objectives: To compare DR-TB treatment outcomes, as defined by the World Health Organization (WHO) at the time of treatment, with simplified definitions.
Methods: We performed retrospective folder reviews of a cohort of 246 South African DR-TB patients, most of whom developed second-line drug resistance. Sequential treatment outcomes were assigned retrospectively using both simplified Tuberculosis Network European Trials Group (TBNET)-based and 2013 WHO-based definitions.
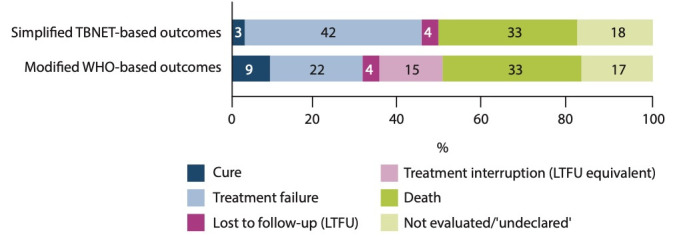
Results: Of 246 patients, 40% were HIV-positive, and 88% developed second-line drug resistance. Patients were observed for a median of 38 (interquartile range 24 - 63) months from DR-TB treatment initiation. Using WHO-based definitions, 93% of patients had >1 sequential outcome, whereas with simplified definitions, 25% of patients had >1 outcome. Fewer outcomes of cure (3% v. 9%) and more outcomes of treatment failure (42% v. 22%) were assigned using simplified definitions.
Conclusion: Simplified outcome definitions applied to real-world patients with long, often complex treatment histories resulted in underestimating cures and overestimating treatment failures compared with WHO-based definitions. Simplified definitions may identify more individuals at higher risk for treatment failure than WHO-based definitions, but without consistent programmatic follow-up it may be difficult to distinguish cure, failure and loss to follow-up.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
