{"title":"Analysis of preoperative risk factors for early recurrence after curative pancreatoduodenectomy for resectable pancreatic adenocarcinoma.","authors":"Pipit Burasakarn, Anuparp Thienhiran, Pusit Fuengfoo, Sermsak Hongjinda","doi":"10.1515/iss-2021-0034","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the risk factors for early recurrence after curative pancreatoduodenectomy for resectable pancreatic ductal adenocarcinoma.</p><p><strong>Methods: </strong>All data were retrospectively collected from patients with resectable pancreatic ductal adenocarcinoma who had undergone pancreatoduodenectomy at the Department of Surgery, Phramongkutklao Hospital, from January 2015 to December 2020. The preoperative and perioperative risk factors were included into the analysis.</p><p><strong>Results: </strong>In total, 34 patients were included in the study. The median time for recurrence and median survival time were 17 and 20 months, respectively. The 1, 3, and 5 year disease-free survival rates were 59.6%, 23.87%, and 23.87%, respectively, while the 1, 3, and 5 year overall survival rates were 81%, 24.7%, and 12.4%, respectively. Seventeen patients (50%) from a total of 34 patients had recurrence, and ten patients (29.41%) had recurrence within 12 months. The independent preoperative risk factor associated with adverse disease-free survival was tumor size > 4 cm (hazard ratio [HR], 14.34, p=0.022). The perioperative risk factors associated with adverse disease-free survival were pathological lymphovascular invasion (HR, 4.31; p=0.048) and non-hepatopancreatobiliary surgeon (HR, 5.9; p=0.022). Risk factors associated with poor overall survival were microscopical margin positive (R1) resection (HR, 3.68; p=0.019) and non-hepatopancreatobiliary surgeon (HR, 3.45; p=0.031).</p><p><strong>Conclusions: </strong>Tumor size > 4 cm from the preoperative imaging study was a poor prognostic factor for early recurrence after curative pancreatoduodenectomy for resectable pancreatic adenocarcinoma indicated that they may have radiological occult metastasis, thus, staging laparoscopy may reduce the number of unnecessary laparotomies and avoid missing radiologically negative metastases.</p>","PeriodicalId":44186,"journal":{"name":"Innovative Surgical Sciences","volume":"7 1","pages":"5-11"},"PeriodicalIF":1.2000,"publicationDate":"2022-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9352185/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovative Surgical Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/iss-2021-0034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/3/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To investigate the risk factors for early recurrence after curative pancreatoduodenectomy for resectable pancreatic ductal adenocarcinoma.
Methods: All data were retrospectively collected from patients with resectable pancreatic ductal adenocarcinoma who had undergone pancreatoduodenectomy at the Department of Surgery, Phramongkutklao Hospital, from January 2015 to December 2020. The preoperative and perioperative risk factors were included into the analysis.
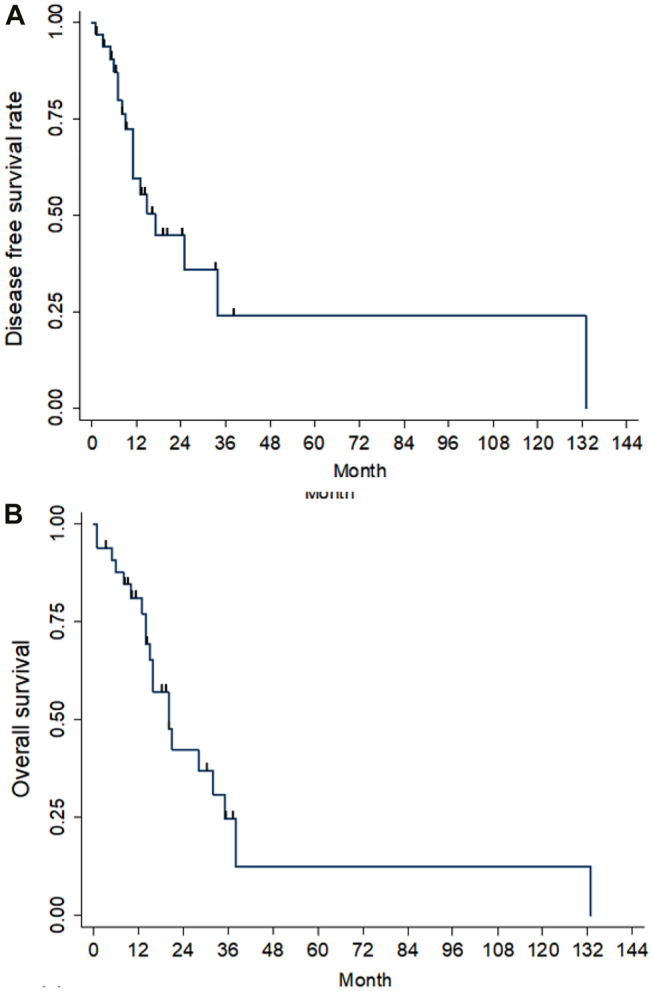
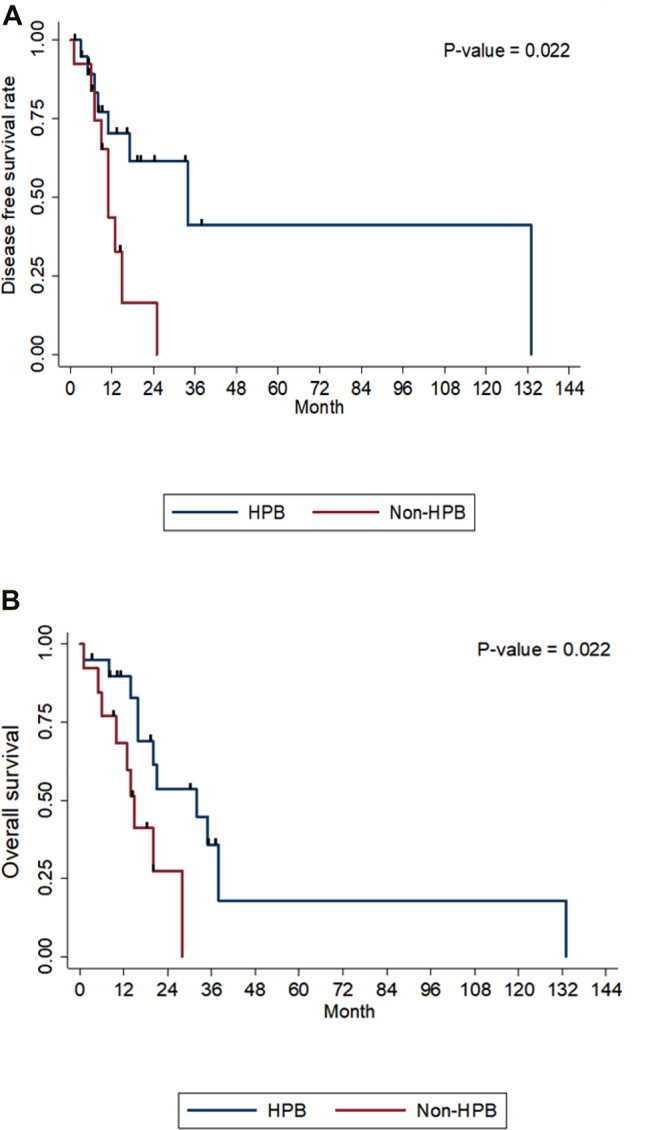
Results: In total, 34 patients were included in the study. The median time for recurrence and median survival time were 17 and 20 months, respectively. The 1, 3, and 5 year disease-free survival rates were 59.6%, 23.87%, and 23.87%, respectively, while the 1, 3, and 5 year overall survival rates were 81%, 24.7%, and 12.4%, respectively. Seventeen patients (50%) from a total of 34 patients had recurrence, and ten patients (29.41%) had recurrence within 12 months. The independent preoperative risk factor associated with adverse disease-free survival was tumor size > 4 cm (hazard ratio [HR], 14.34, p=0.022). The perioperative risk factors associated with adverse disease-free survival were pathological lymphovascular invasion (HR, 4.31; p=0.048) and non-hepatopancreatobiliary surgeon (HR, 5.9; p=0.022). Risk factors associated with poor overall survival were microscopical margin positive (R1) resection (HR, 3.68; p=0.019) and non-hepatopancreatobiliary surgeon (HR, 3.45; p=0.031).
Conclusions: Tumor size > 4 cm from the preoperative imaging study was a poor prognostic factor for early recurrence after curative pancreatoduodenectomy for resectable pancreatic adenocarcinoma indicated that they may have radiological occult metastasis, thus, staging laparoscopy may reduce the number of unnecessary laparotomies and avoid missing radiologically negative metastases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
