IGH/BCL2 Status Better Predicts Clinico-Pathological Behavior in Primary Splenic Follicular Lymphoma than Histological Grade and Other Molecular Markers.
{"title":"IGH/BCL2 Status Better Predicts Clinico-Pathological Behavior in Primary Splenic Follicular Lymphoma than Histological Grade and Other Molecular Markers.","authors":"Cherian Verghese, Weihong Li, Nanuli Gvazava, Emmanouil Alimpertis, Navkirat Kahlon, Hongliu Sun, Robert Booth","doi":"10.1177/2632010X221129242","DOIUrl":null,"url":null,"abstract":"<p><p>Splenic lymphoma may be primary or secondary. Primary splenic lymphoma's are rare and usually of follicular cell origin representing <1% of Non-Hodgkin's Lymphoma's. Most are secondary with 35% representing Marginal Cell sub-type with the rest being Diffuse Large B-Cell Lymphoma's. Unlike the uniformly aggressive clinical course of Diffuse Large B-Cell Lymphoma's, biological behavior of Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma remains less well defined. We present here a solitary splenic mass confirmed as Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma after a diagnostic splenectomy. Biopsy revealed monomorphic small lymphoid cells with low grade mitotic activity. Flow cytometry showed a lambda restricted population of B-Cells displaying dim CD19 and CD10. The cells were negative for CD5, CD11c, and CD103. FISH was negative for IGH/BCL2 fusion unlike nodal Follicular Lymphoma's which are usually positive for this translocation. Evidence from this case and a review of literature support the finding that Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma is less likely to have the classic IGH-BCL2 fusion and the associated chromosomal 14;18 translocation. This profile is associated with less aggressive clinical behavior even when histopathology represents a high-grade pattern. In such cases splenectomy alone is adequate for localized disease when negative for IGH/BCL2 fusion regardless of histological grade.</p>","PeriodicalId":53204,"journal":{"name":"Clinical Pathology","volume":" ","pages":"2632010X221129242"},"PeriodicalIF":1.9000,"publicationDate":"2022-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/91/8b/10.1177_2632010X221129242.PMC9608027.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pathology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2632010X221129242","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
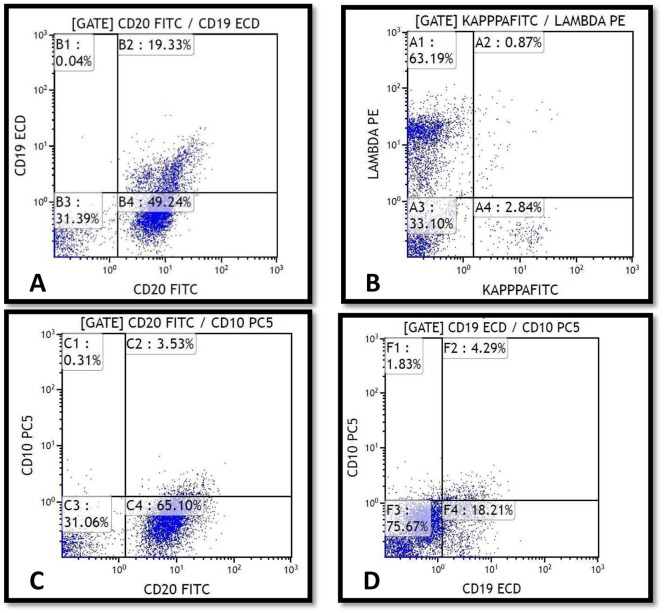
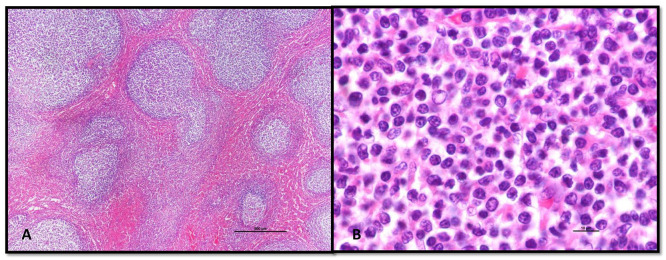
Splenic lymphoma may be primary or secondary. Primary splenic lymphoma's are rare and usually of follicular cell origin representing <1% of Non-Hodgkin's Lymphoma's. Most are secondary with 35% representing Marginal Cell sub-type with the rest being Diffuse Large B-Cell Lymphoma's. Unlike the uniformly aggressive clinical course of Diffuse Large B-Cell Lymphoma's, biological behavior of Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma remains less well defined. We present here a solitary splenic mass confirmed as Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma after a diagnostic splenectomy. Biopsy revealed monomorphic small lymphoid cells with low grade mitotic activity. Flow cytometry showed a lambda restricted population of B-Cells displaying dim CD19 and CD10. The cells were negative for CD5, CD11c, and CD103. FISH was negative for IGH/BCL2 fusion unlike nodal Follicular Lymphoma's which are usually positive for this translocation. Evidence from this case and a review of literature support the finding that Primary Splenic CD10-Positive Small B-Cell Lymphoma/Follicular Lymphoma is less likely to have the classic IGH-BCL2 fusion and the associated chromosomal 14;18 translocation. This profile is associated with less aggressive clinical behavior even when histopathology represents a high-grade pattern. In such cases splenectomy alone is adequate for localized disease when negative for IGH/BCL2 fusion regardless of histological grade.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
