Interpleural location of chest drain on ultrasound excludes pneumothorax and associates with a low degree of chest drain foreshortening on the antero-posterior chest X-ray.
Michal Maly, Masego Candy Mokotedi, Eva Svobodova, Marek Flaksa, Michal Otahal, Zdenek Stach, Jan Rulisek, Tomas Brozek, Michal Porizka, Martin Balik
{"title":"Interpleural location of chest drain on ultrasound excludes pneumothorax and associates with a low degree of chest drain foreshortening on the antero-posterior chest X-ray.","authors":"Michal Maly, Masego Candy Mokotedi, Eva Svobodova, Marek Flaksa, Michal Otahal, Zdenek Stach, Jan Rulisek, Tomas Brozek, Michal Porizka, Martin Balik","doi":"10.1186/s13089-022-00296-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of chest drain (CD) location by bedside imaging methods in the diagnosis of pneumothorax has not been explored in a prospective study yet.</p><p><strong>Methods: </strong>Covid-19 ARDS patients with pneumothorax were prospectively monitored with chest ultrasound (CUS) and antero-posterior X-ray (CR) performed after drainage in the safe triangle. CD foreshortening was estimated as a decrease of chest drain index (CDI = length of CD in chest taken from CR/depth of insertion on CD scale + 5 cm). The angle of inclination of the CD was measured between the horizontal line and the CD at the point where it enters pleural space on CR.</p><p><strong>Results: </strong>Of the total 106 pneumothorax cases 80 patients had full lung expansion on CUS, the CD was located by CUS in 69 (86%), the CDI was 0.99 (0.88-1.06). 26 cases had a residual pneumothorax after drainage (24.5%), the CD was located by CUS in 31%, the CDI was 0.76 (0.6-0.93),p < 0.01. The risk ratio for a pneumothorax in a patient with not visible CD between the pleural layers on CUS and an associated low CDI on CR was 5.97, p˂0.0001. For the patients with a steep angle of inclination (> 50°) of the CD, the risk ratio for pneumothorax was not significant (p < 0.17). A continued air leak from the CD after drainage is related to the risk for a residual pneumothorax (RR 2.27, p = 0.003).</p><p><strong>Conclusion: </strong>Absence of a CD on CUS post drainage, low CDI on CR and continuous air leak significantly associate with residual occult pneumothorax which may evade diagnosis on an antero-posterior CR.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":" ","pages":"45"},"PeriodicalIF":2.9000,"publicationDate":"2022-11-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9670049/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-022-00296-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
Abstract
Background: The role of chest drain (CD) location by bedside imaging methods in the diagnosis of pneumothorax has not been explored in a prospective study yet.
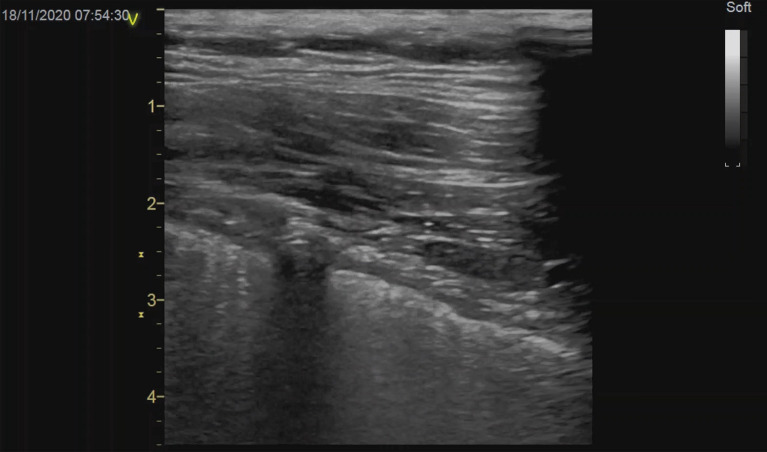
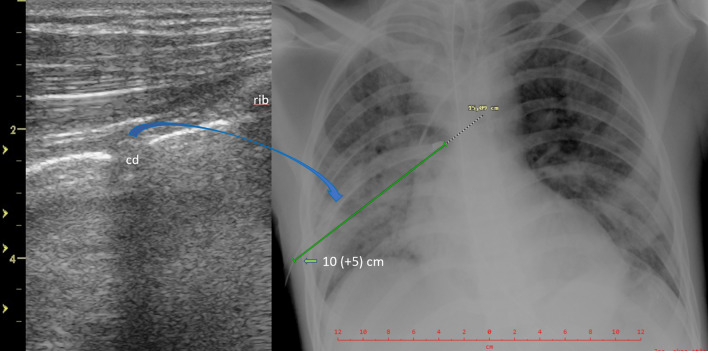
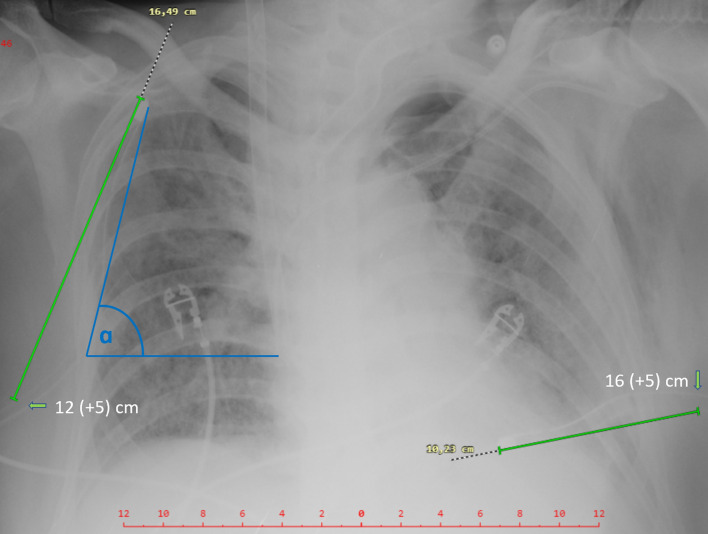
Methods: Covid-19 ARDS patients with pneumothorax were prospectively monitored with chest ultrasound (CUS) and antero-posterior X-ray (CR) performed after drainage in the safe triangle. CD foreshortening was estimated as a decrease of chest drain index (CDI = length of CD in chest taken from CR/depth of insertion on CD scale + 5 cm). The angle of inclination of the CD was measured between the horizontal line and the CD at the point where it enters pleural space on CR.
Results: Of the total 106 pneumothorax cases 80 patients had full lung expansion on CUS, the CD was located by CUS in 69 (86%), the CDI was 0.99 (0.88-1.06). 26 cases had a residual pneumothorax after drainage (24.5%), the CD was located by CUS in 31%, the CDI was 0.76 (0.6-0.93),p < 0.01. The risk ratio for a pneumothorax in a patient with not visible CD between the pleural layers on CUS and an associated low CDI on CR was 5.97, p˂0.0001. For the patients with a steep angle of inclination (> 50°) of the CD, the risk ratio for pneumothorax was not significant (p < 0.17). A continued air leak from the CD after drainage is related to the risk for a residual pneumothorax (RR 2.27, p = 0.003).
Conclusion: Absence of a CD on CUS post drainage, low CDI on CR and continuous air leak significantly associate with residual occult pneumothorax which may evade diagnosis on an antero-posterior CR.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
