Annekatrin Schulze, Jurek Schultz, Adrian Dragu, Guido Fitze
{"title":"Diagnostics and Treatment of Volkmann Ischemic Contracture in a Seven-Year-Old Child.","authors":"Annekatrin Schulze, Jurek Schultz, Adrian Dragu, Guido Fitze","doi":"10.1055/s-0042-1749210","DOIUrl":null,"url":null,"abstract":"<p><p>A 7-year-old boy presented 6 weeks after open reduction and crossed Kirschner wire (K-wire) fixation of a supracondylar humerus fracture. Previous treatments had restored skeletal anatomy without documented complications. However, the patient would not move the entire arm, including his forearm and hand. Any passive movement led to anxious adverse reactions, and there was partial numbness of all fingers. After intensive physio- and occupational therapy supported by nerve stimulation and psychological counseling, anxiety-related functional deficits of the shoulder and elbow resolved to reveal the severe Volkmann contracture of the right hand developed fully. Electroneurography, X-ray, magnetic resonance imaging of the forearm, and ultrasonography showed nonfunctional ulnar and a partially disturbed radial motor nerve distal to the elbow along with damaged flexor muscles of the forearm after compartment syndrome. In addition, damage to the median nerve at the elbow level was diagnosed. After intense conservative therapy, we partially resected fibrotic fascia of the superficial flexor compartment, freed ulnar and median nerves, and performed staircase-like releases of tendons and tenotomies. We achieved a full range of motion of all fingers and markedly improved the range of motion of the wrist. The Disabilities of the Arm, Shoulder and Hand scores for function improved from 80 to 16 at the 2-year follow-up postoperatively, but some impairments of fine motor function persisted. Subtle symptoms of a developing compartment syndrome need to be recognized. Overlooked and untreated, a consecutive Volkmann contracture can turn the extremity nonfunctional. Intensive physical, psychological, and surgical therapy in a specialized center can restore function but requires endurance and perseverance throughout the lengthy recovery.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":" ","pages":"e68-e72"},"PeriodicalIF":0.7000,"publicationDate":"2022-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9296264/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1749210","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 1
Abstract
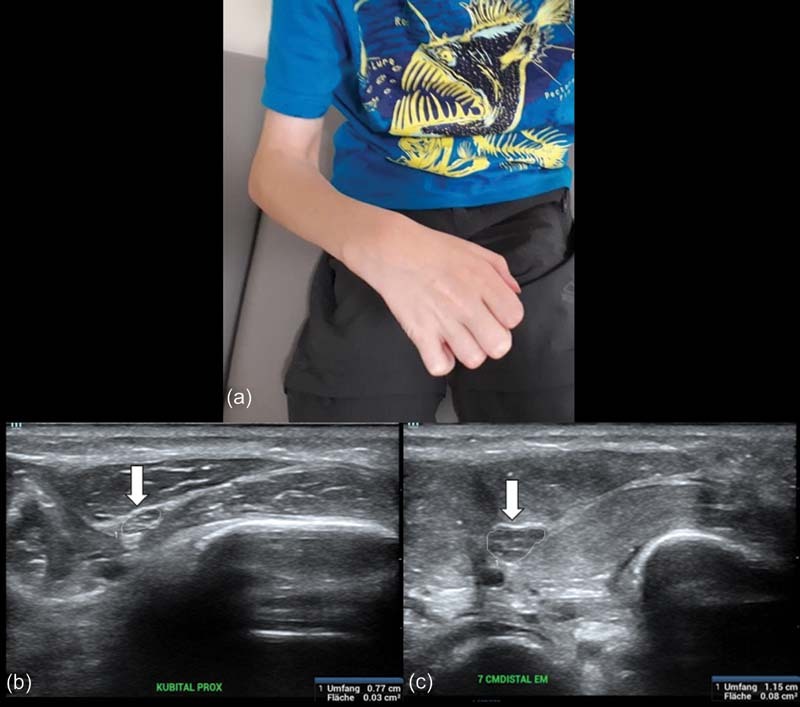
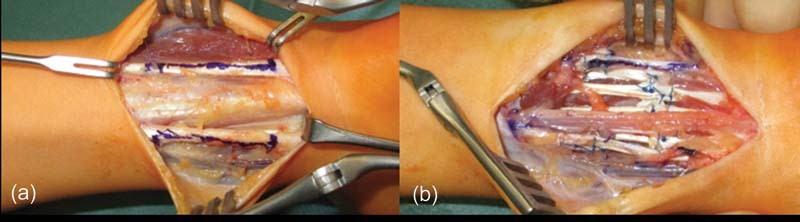
A 7-year-old boy presented 6 weeks after open reduction and crossed Kirschner wire (K-wire) fixation of a supracondylar humerus fracture. Previous treatments had restored skeletal anatomy without documented complications. However, the patient would not move the entire arm, including his forearm and hand. Any passive movement led to anxious adverse reactions, and there was partial numbness of all fingers. After intensive physio- and occupational therapy supported by nerve stimulation and psychological counseling, anxiety-related functional deficits of the shoulder and elbow resolved to reveal the severe Volkmann contracture of the right hand developed fully. Electroneurography, X-ray, magnetic resonance imaging of the forearm, and ultrasonography showed nonfunctional ulnar and a partially disturbed radial motor nerve distal to the elbow along with damaged flexor muscles of the forearm after compartment syndrome. In addition, damage to the median nerve at the elbow level was diagnosed. After intense conservative therapy, we partially resected fibrotic fascia of the superficial flexor compartment, freed ulnar and median nerves, and performed staircase-like releases of tendons and tenotomies. We achieved a full range of motion of all fingers and markedly improved the range of motion of the wrist. The Disabilities of the Arm, Shoulder and Hand scores for function improved from 80 to 16 at the 2-year follow-up postoperatively, but some impairments of fine motor function persisted. Subtle symptoms of a developing compartment syndrome need to be recognized. Overlooked and untreated, a consecutive Volkmann contracture can turn the extremity nonfunctional. Intensive physical, psychological, and surgical therapy in a specialized center can restore function but requires endurance and perseverance throughout the lengthy recovery.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
