Potential Applicability of Local Resection With Prophylactic Left Gastric Artery Basin Dissection for Early-Stage Gastric Cancer in the Upper Third of the Stomach.
{"title":"Potential Applicability of Local Resection With Prophylactic Left Gastric Artery Basin Dissection for Early-Stage Gastric Cancer in the Upper Third of the Stomach.","authors":"Yoshimasa Akashi, Koichi Ogawa, Katsuji Hisakura, Tsuyoshi Enomoto, Yusuke Ohara, Yohei Owada, Shinji Hashimoto, Kazuhiro Takahashi, Osamu Shimomura, Manami Doi, Yoshihiro Miyazaki, Kinji Furuya, Shoko Moue, Tatsuya Oda","doi":"10.5230/jgc.2022.22.e17","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Total or proximal gastrectomy of the upper-third early gastric cancer (u-EGC) often causes severe post-gastrectomy syndrome, suggesting that these procedures are extremely invasive for patients without pathologically positive lymph node (LN) metastasis. This study aimed to evaluate the clinical applicability of a stomach function-preserving surgery, local resection (LR), with prophylactic left gastric artery (LGA)-basin dissection (LGA-BD).</p><p><strong>Materials and methods: </strong>The data of patients with u-EGC (pathologically diagnosed as T1) were retrospectively analyzed. Total gastrectomy was performed in 30 patients, proximal gastrectomy in 45, and subtotal gastrectomy in 6; the LN status was evaluated assuming that the patients had already underwent LR + LGA-BD. This procedure was considered feasible in patients without LN metastases or in patients with cancer in the LGA basin. The reproducibility of the results was also evaluated using an external validation dataset.</p><p><strong>Results: </strong>Of the 82 eligible patients, 79 (96.3%) were cured after undergoing LR + LGA-BD, 74 (90.2%) were pathologically negative for LN metastases, and 5 (6.1%) had LN metastases, but these findings were only observed in the LGA basin. Similarly, of the 406 eligible tumors in the validation dataset, 396 (97.5%) were potentially curative. Tumors in the lesser curvature, post-endoscopic resection status, and small tumors (<20 mm) were considered to be stronger indicators of LR + LGA-BD as all subpopulation cases met our feasibility criteria.</p><p><strong>Conclusions: </strong>More than 95% of the patients with u-EGC might be eligible for LR + LGA-BD. This function-preserving procedure may contribute to the development of u-EGC without pathological LN metastases, especially for tumors located at the lesser curvature.</p>","PeriodicalId":56072,"journal":{"name":"Journal of Gastric Cancer","volume":"22 3","pages":"184-196"},"PeriodicalIF":3.8000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/38/jgc-22-184.PMC9359880.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastric Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5230/jgc.2022.22.e17","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
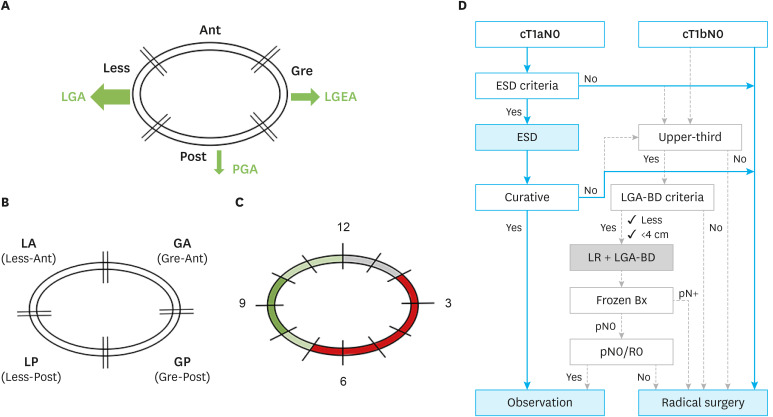
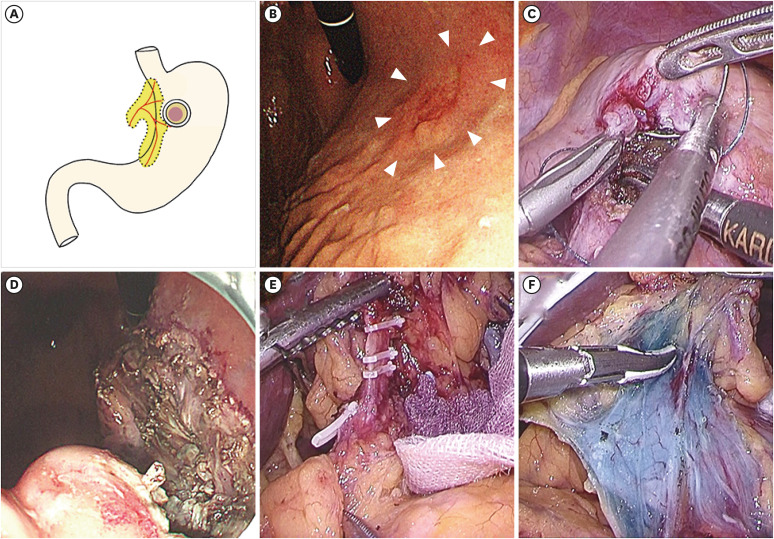
Purpose: Total or proximal gastrectomy of the upper-third early gastric cancer (u-EGC) often causes severe post-gastrectomy syndrome, suggesting that these procedures are extremely invasive for patients without pathologically positive lymph node (LN) metastasis. This study aimed to evaluate the clinical applicability of a stomach function-preserving surgery, local resection (LR), with prophylactic left gastric artery (LGA)-basin dissection (LGA-BD).
Materials and methods: The data of patients with u-EGC (pathologically diagnosed as T1) were retrospectively analyzed. Total gastrectomy was performed in 30 patients, proximal gastrectomy in 45, and subtotal gastrectomy in 6; the LN status was evaluated assuming that the patients had already underwent LR + LGA-BD. This procedure was considered feasible in patients without LN metastases or in patients with cancer in the LGA basin. The reproducibility of the results was also evaluated using an external validation dataset.
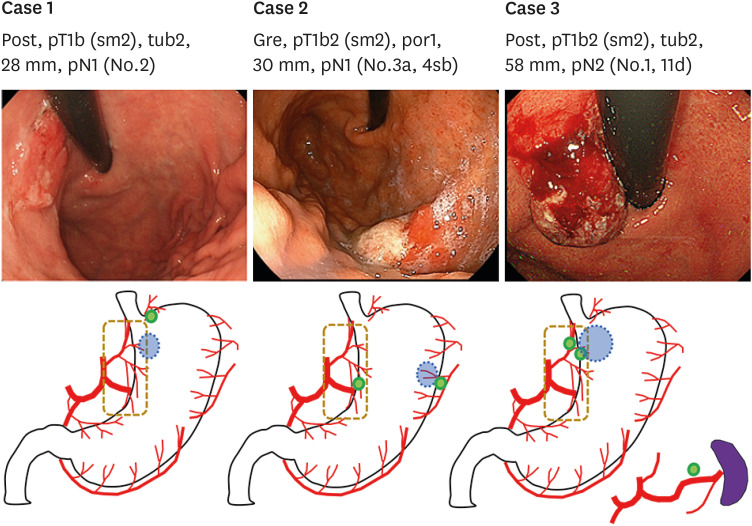
Results: Of the 82 eligible patients, 79 (96.3%) were cured after undergoing LR + LGA-BD, 74 (90.2%) were pathologically negative for LN metastases, and 5 (6.1%) had LN metastases, but these findings were only observed in the LGA basin. Similarly, of the 406 eligible tumors in the validation dataset, 396 (97.5%) were potentially curative. Tumors in the lesser curvature, post-endoscopic resection status, and small tumors (<20 mm) were considered to be stronger indicators of LR + LGA-BD as all subpopulation cases met our feasibility criteria.
Conclusions: More than 95% of the patients with u-EGC might be eligible for LR + LGA-BD. This function-preserving procedure may contribute to the development of u-EGC without pathological LN metastases, especially for tumors located at the lesser curvature.
期刊介绍:
The Journal of Gastric Cancer (J Gastric Cancer) is an international peer-reviewed journal. Each issue carries high quality clinical and translational researches on gastric neoplasms. Editorial Board of J Gastric Cancer publishes original articles on pathophysiology, molecular oncology, diagnosis, treatment, and prevention of gastric cancer as well as articles on dietary control and improving the quality of life for gastric cancer patients. J Gastric Cancer includes case reports, review articles, how I do it articles, editorials, and letters to the editor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
