Henry H L Wu, Claire C Y Wang, Alexander Woywodt, Arvind Ponnusamy
{"title":"Concurrent presentation of IgG4-related tubulointerstitial nephritis and ANCA MPO crescentic glomerulonephritis.","authors":"Henry H L Wu, Claire C Y Wang, Alexander Woywodt, Arvind Ponnusamy","doi":"10.5414/CNCS110852","DOIUrl":null,"url":null,"abstract":"<p><p>Concurrent IgG4-related tubulointerstitial nephritis and anti-neutrophil cytoplasmic antibodies (ANCA) myeloperoxidase (MPO) crescentic glomerulonephritis is an uncommon scenario, and the link between the two conditions, if any, is incompletely understood. We report the case of a 58-year-old woman who presented with a 2-month history of malaise and joint pain and was found to have acute kidney injury and hemato-proteinuria. Initial immunological tests revealed positive anti-neutrophil cytoplasmic antibodies with a peri-nuclear pattern (pANCA). An enzyme-linked immunoassay (ELISA) for anti-MPO antibodies was also positive, leading to a tentative diagnosis of ANCA-associated small vessel vasculitis with renal involvement. Steroid treatment was commenced, and an urgent kidney biopsy was performed. This showed crescentic glomerulonephritis, but also demonstrated concurrent tubulointerstitial nephritis with a dominance of IgG4-producing plasma cells. Serum IgG4 levels were also elevated. The patient was initially treated with intravenous cyclophosphamide and steroids and then switched to rituximab. When last seen, she was well after 1 dose of rituximab, with kidney function, inflammatory parameters, and serum IgG4 levels returning to normal levels. The concurrent presentation of ANCA-associated vasculitis and IgG4 renal disease is rare with only few cases reported in the literature. More work is needed to understand pathophysiology, outcomes, and management options for this complex scenario.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":" ","pages":"47-53"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9275406/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110852","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
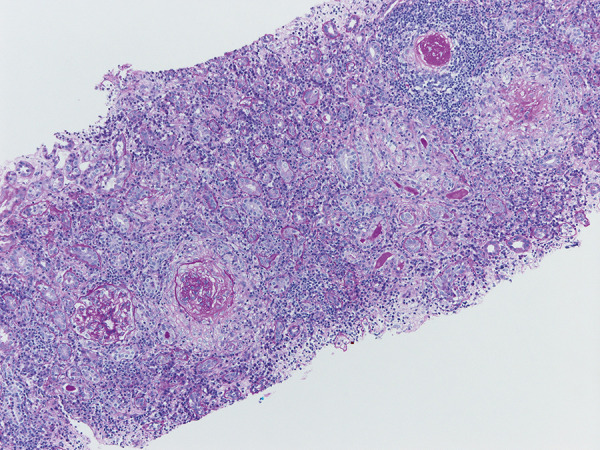
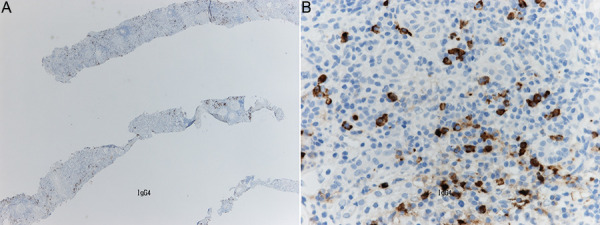
Concurrent IgG4-related tubulointerstitial nephritis and anti-neutrophil cytoplasmic antibodies (ANCA) myeloperoxidase (MPO) crescentic glomerulonephritis is an uncommon scenario, and the link between the two conditions, if any, is incompletely understood. We report the case of a 58-year-old woman who presented with a 2-month history of malaise and joint pain and was found to have acute kidney injury and hemato-proteinuria. Initial immunological tests revealed positive anti-neutrophil cytoplasmic antibodies with a peri-nuclear pattern (pANCA). An enzyme-linked immunoassay (ELISA) for anti-MPO antibodies was also positive, leading to a tentative diagnosis of ANCA-associated small vessel vasculitis with renal involvement. Steroid treatment was commenced, and an urgent kidney biopsy was performed. This showed crescentic glomerulonephritis, but also demonstrated concurrent tubulointerstitial nephritis with a dominance of IgG4-producing plasma cells. Serum IgG4 levels were also elevated. The patient was initially treated with intravenous cyclophosphamide and steroids and then switched to rituximab. When last seen, she was well after 1 dose of rituximab, with kidney function, inflammatory parameters, and serum IgG4 levels returning to normal levels. The concurrent presentation of ANCA-associated vasculitis and IgG4 renal disease is rare with only few cases reported in the literature. More work is needed to understand pathophysiology, outcomes, and management options for this complex scenario.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
