Combined Liver Stiffness and Α-fetoprotein Further beyond the Sustained Virologic Response Visit as Predictors of Long-Term Liver-Related Events in Patients with Chronic Hepatitis C.
{"title":"Combined Liver Stiffness and Α-fetoprotein Further beyond the Sustained Virologic Response Visit as Predictors of Long-Term Liver-Related Events in Patients with Chronic Hepatitis C.","authors":"Sheng-Hung Chen, Hsueh-Chou Lai, Wen-Pang Su, Jung-Ta Kao, Po-Heng Chuang, Wei-Fan Hsu, Hung-Wei Wang, Tsung-Lin Hsieh, Hung-Yao Chen, Cheng-Yuan Peng","doi":"10.1155/2022/5201443","DOIUrl":null,"url":null,"abstract":"Aims Long-term risk stratification using combined liver stiffness (LS) and clinically relevant blood tests acquired at the baseline further beyond the sustained virologic response (SVR) visit for chronic hepatitis C (CHC) has not been thoroughly investigated. This study retrospectively investigated the prognostics of liver-related events (LREs) further beyond the SVR visit. Methods Cox regression and random forest models identified the key factors, including longitudinal LS and noninvasive test results, that could predict LREs, including hepatocellular carcinoma, during prespecified follow-ups from 2010 to 2021. Kaplan–Meier survival analysis estimated the significance of between-group risk stratification. Results Of the entire eligible cohort (n = 520) of CHC patients with SVR to antiviral therapy, 28 (5.4%) patients developed post-SVR LREs over a median follow-up period of 6.1 years (interquartile range = 3.5–8.7). The multivariate Cox regression analysis identified two significant predictors of LREs after the year 3 post-SVR (Y3PSVR) baseline (LRE, n = 15 of 28, 53.6%, median follow-up = 4.1 [1.6–6.4] years after Y3PSVR): LS at Y3PSVR (adjusted hazard ratio [aHR] = 3.980, 95% confidence interval [CI] = 2.085–7.597, P < 0.001), and α-fetoprotein (AFP) at Y3PSVR (aHR = 1.017, 95% CI = 1.001–1.034, P=0.034). LS ≥1.45 m/s and AFP ≥3.00 ng/mL for Y3PSVR yielded positive likelihood ratios of 4.24 and 2.62, respectively. Kaplan–Meier analysis revealed that among the stratified subgroups, the subgroup with concurrent LS ≥1.45 m/s and AFP ≥3.00 ng/mL at Y3PSVR exhibited the highest risk of LREs after Y3PSVR (log-rank P < 0.001). Conclusion We recommend the combined use of concurrent LS and AFP in future prediction models for LREs in CHC. Patients with concurrently high LS and AFP values further beyond the SVR visit may require a recall policy involving intense surveillance.","PeriodicalId":48755,"journal":{"name":"Canadian Journal of Gastroenterology and Hepatology","volume":" ","pages":"5201443"},"PeriodicalIF":2.3000,"publicationDate":"2022-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9273470/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2022/5201443","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
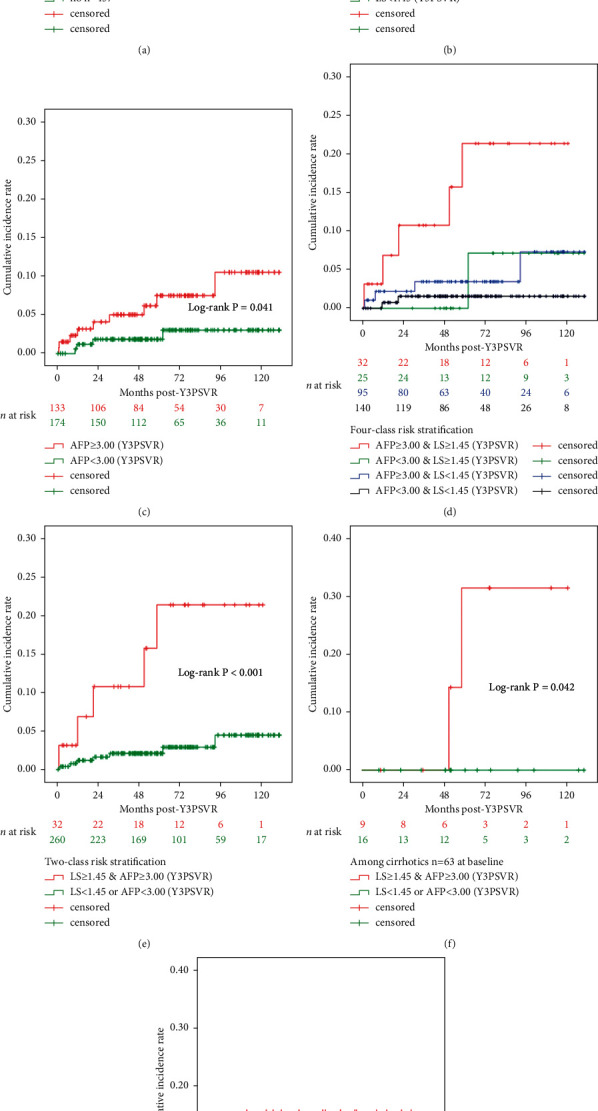
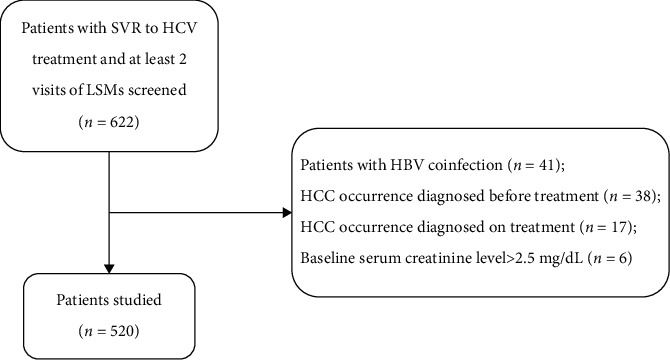
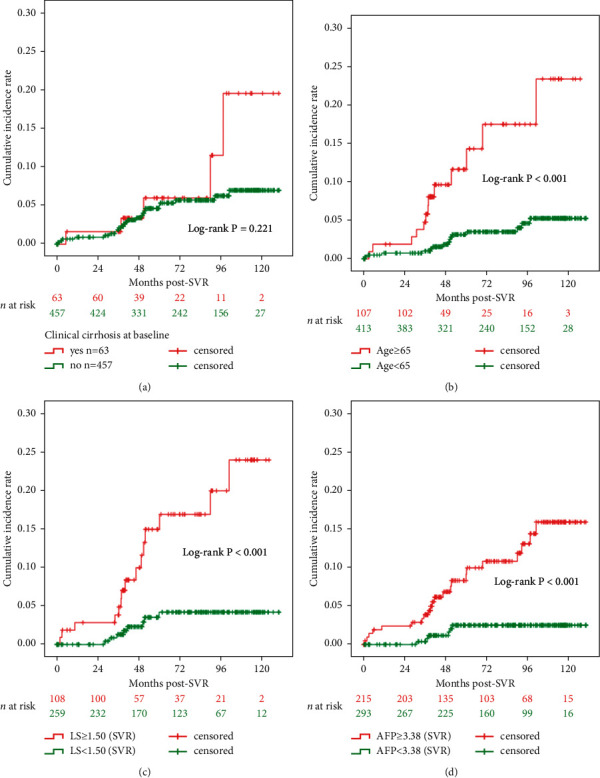
Aims Long-term risk stratification using combined liver stiffness (LS) and clinically relevant blood tests acquired at the baseline further beyond the sustained virologic response (SVR) visit for chronic hepatitis C (CHC) has not been thoroughly investigated. This study retrospectively investigated the prognostics of liver-related events (LREs) further beyond the SVR visit. Methods Cox regression and random forest models identified the key factors, including longitudinal LS and noninvasive test results, that could predict LREs, including hepatocellular carcinoma, during prespecified follow-ups from 2010 to 2021. Kaplan–Meier survival analysis estimated the significance of between-group risk stratification. Results Of the entire eligible cohort (n = 520) of CHC patients with SVR to antiviral therapy, 28 (5.4%) patients developed post-SVR LREs over a median follow-up period of 6.1 years (interquartile range = 3.5–8.7). The multivariate Cox regression analysis identified two significant predictors of LREs after the year 3 post-SVR (Y3PSVR) baseline (LRE, n = 15 of 28, 53.6%, median follow-up = 4.1 [1.6–6.4] years after Y3PSVR): LS at Y3PSVR (adjusted hazard ratio [aHR] = 3.980, 95% confidence interval [CI] = 2.085–7.597, P < 0.001), and α-fetoprotein (AFP) at Y3PSVR (aHR = 1.017, 95% CI = 1.001–1.034, P=0.034). LS ≥1.45 m/s and AFP ≥3.00 ng/mL for Y3PSVR yielded positive likelihood ratios of 4.24 and 2.62, respectively. Kaplan–Meier analysis revealed that among the stratified subgroups, the subgroup with concurrent LS ≥1.45 m/s and AFP ≥3.00 ng/mL at Y3PSVR exhibited the highest risk of LREs after Y3PSVR (log-rank P < 0.001). Conclusion We recommend the combined use of concurrent LS and AFP in future prediction models for LREs in CHC. Patients with concurrently high LS and AFP values further beyond the SVR visit may require a recall policy involving intense surveillance.
期刊介绍:
Canadian Journal of Gastroenterology and Hepatology is a peer-reviewed, open access journal that publishes original research articles, review articles, and clinical studies in all areas of gastroenterology and liver disease - medicine and surgery.
The Canadian Journal of Gastroenterology and Hepatology is sponsored by the Canadian Association of Gastroenterology and the Canadian Association for the Study of the Liver.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
