{"title":"Diagnostic accuracy and prognostic value of lung ultrasound in coronavirus disease (COVID-19).","authors":"Javid Azadbakht, Maryam Saffari, Hamidreza Talarie, Mahsa Masjedi Esfahani, Mahdi Barzegar","doi":"10.5114/pjr.2022.118304","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to assess the correlation between lung ultrasound (LUS) and computed tomography (CT) findings and the predictability of LUS scores to anticipate disease characteristics, lab data, clinical severity, and mortality in patients with COVID-19.</p><p><strong>Material and methods: </strong>Fifty consecutive hospitalized PCR-confirmed COVID-19 patients who underwent chest CT scan and LUS on the first day of admission were enrolled. The LUS score was calculated based on the presence, severity, and distribution of parenchymal abnormalities in 14 regions.</p><p><strong>Results: </strong>The participants' mean age was 54.60 ± 19.93 years, and 26 (52%) were female. All patients had CT and LUS findings typical of COVID-19. The mean value of CT and LUS severity scores were 11.80 ± 3.89 (ranging from 2 to 20) and 13.74 ± 6.43 (ranging from 1 to 29), respectively. The LUS score was significantly higher in females (<i>p</i> = 0.016), and patients with dyspnoea (<i>p</i> = 0.048), HTN (<i>p</i> = 0.034), immunodeficiency (<i>p</i> = 0.034), room air SpO<sub>2</sub> ≤ 93 (<i>p</i> = 0.02), and pleural effusion (<i>p</i> = 0.036). LUS findings were strongly correlated with CT scan results regarding lesion type, distribution, and severity in a region-by-region fashion (92-100% agreement). An LUS score of 14 or higher was predictive of room air SpO<sub>2</sub> ≤ 93 and ICU admission, while an LUS score ≥ 12 was predictive of death (<i>p</i> = 0.011, 0.023, and 0.003, respectively).</p><p><strong>Conclusions: </strong>Our results suggested that LUS can be used as a valuable tool for detecting COVID-19 pneumonia and determining high-risk hospitalized patients, helping to triage and stratify high-risk patients, which waives the need to undertake irradiating chest CT and reduces the burden of overworked CT department staff.</p>","PeriodicalId":47128,"journal":{"name":"Polish Journal of Radiology","volume":" ","pages":"e397-e408"},"PeriodicalIF":1.6000,"publicationDate":"2022-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/e2/PJR-87-47545.PMC9373868.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Polish Journal of Radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pjr.2022.118304","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: This study aimed to assess the correlation between lung ultrasound (LUS) and computed tomography (CT) findings and the predictability of LUS scores to anticipate disease characteristics, lab data, clinical severity, and mortality in patients with COVID-19.
Material and methods: Fifty consecutive hospitalized PCR-confirmed COVID-19 patients who underwent chest CT scan and LUS on the first day of admission were enrolled. The LUS score was calculated based on the presence, severity, and distribution of parenchymal abnormalities in 14 regions.
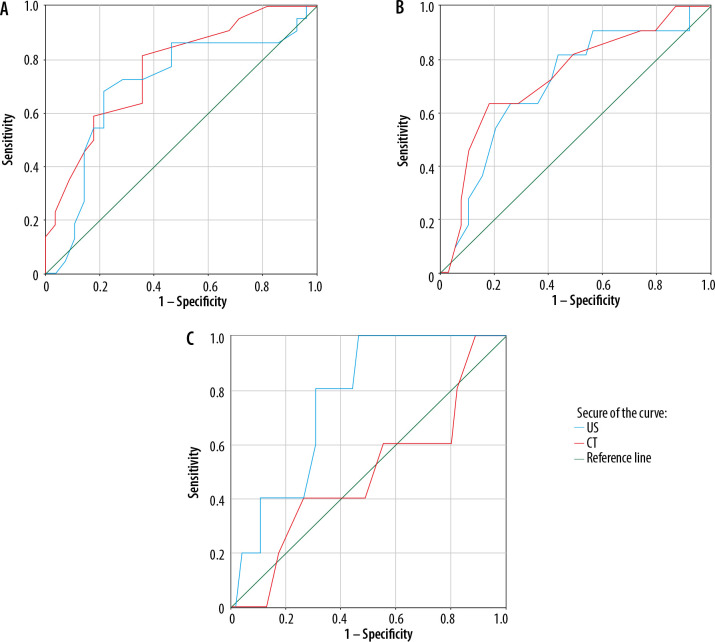
Results: The participants' mean age was 54.60 ± 19.93 years, and 26 (52%) were female. All patients had CT and LUS findings typical of COVID-19. The mean value of CT and LUS severity scores were 11.80 ± 3.89 (ranging from 2 to 20) and 13.74 ± 6.43 (ranging from 1 to 29), respectively. The LUS score was significantly higher in females (p = 0.016), and patients with dyspnoea (p = 0.048), HTN (p = 0.034), immunodeficiency (p = 0.034), room air SpO2 ≤ 93 (p = 0.02), and pleural effusion (p = 0.036). LUS findings were strongly correlated with CT scan results regarding lesion type, distribution, and severity in a region-by-region fashion (92-100% agreement). An LUS score of 14 or higher was predictive of room air SpO2 ≤ 93 and ICU admission, while an LUS score ≥ 12 was predictive of death (p = 0.011, 0.023, and 0.003, respectively).
Conclusions: Our results suggested that LUS can be used as a valuable tool for detecting COVID-19 pneumonia and determining high-risk hospitalized patients, helping to triage and stratify high-risk patients, which waives the need to undertake irradiating chest CT and reduces the burden of overworked CT department staff.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
